Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Aktuality ve farmakoterapii diabetu
Marek Honka Diabetologické centrum FN Ostrava

2
Přehled sdělení Strategie léčby diabetu 2.typu
Účinky metforminu mimo metabolismus sacharidů Léčiva odvozená od účinku inkretinů Perspektiva glitazonů po „pádu“ rosiglitazonu

3
Reflexe výsledků UKPDS-ACCORD-ADVANCE v současné strategii léčby DM 2
Reflexe výsledků UKPDS-ACCORD-ADVANCE v současné strategii léčby DM 2.typu prokázán dlouhodobý efekt kompenzace i pro diabetes 2.typu intenzivní intervence od začátku onemocnění nejefektivnější opožděná intervence nesmí být spojena s nárůstem rizika hypoglykémie

4
Intervence ve vztahu ke KVS riziku
přínos jednotlivých intervencí se u DM 2. typu sčítá účinek intervence narůstá s časem (lineárně - exponenciálně?) z intenzivní léčby profitují zejména osoby: s nižším vstupním HbA1c s kratším trváním diabetu bez přítomnosti mikro a makrovaskulárního postižení
 z intenzivní léčby profitují zejména osoby: s nižším vstupním HbA1c. s kratším trváním diabetu. bez přítomnosti mikro a makrovaskulárního postižení.")
6
Intervence ve vztahu ke KVS riziku
U osob s poškozeným cévním řečištěm ani sebelepší instrumentální výkon příliš nezlepší prognosu quo ad vitam

7
Nová data o metforminu

8
Účinek metforminu na HbA1C a lipidogram: meta-analýza 41 studií
Průměrná změna při terapii metforminem (95% CI) p HbA1C (%) -0,74 (-0.84 to -0.65) < Triglyceridy (mmol/l) -0,13 (-0.21 to -0.04) 0.003 celkový cholesterol (mmol/l) -0,26 (-0.34 to -0.18) <0.0001 LDL-cholesterol (mmol/l) -0,22 (-0.31 to -0.13) HDL-cholesterol (mmol/l) 0,01 (-0.02 to -0.03) 0.50 Effects of metformin on glycaemia and lipids: data from a meta-analysis These data are from a meta-analysis of 41 studies of at least 6 weeks’ duration providing data on glycaemia, lipids and/or blood pressure in patients treated with metformin. Metformin treatment was associated with significant reductions in HbA1C, triglycerides, total cholesterol and LDL-cholesterol. HDL-cholesterol was unaffected. Metformin also did not affect systolic blood pressure (mean change mmHg [95% CI to 0.82] or diastolic blood pressure (mean change [95% CI to -0.21]). Wulffele MG, Kooy A, de Zeeuw D, Stehouwer CD, Gansevoort RT. The effect of metformin on blood pressure, plasma cholesterol and triglycerides in type 2 diabetes mellitus: a systematic review. J Intern Med 2004;256:1-14 Wulffele MG et al. J Intern Med 2004;256:1-14
 p. HbA1C (%) -0,74 (-0.84 to -0.65) < Triglyceridy (mmol/l) -0,13 (-0.21 to -0.04) celkový cholesterol (mmol/l) -0,26 (-0.34 to -0.18) < LDL-cholesterol (mmol/l) -0,22 (-0.31 to -0.13) HDL-cholesterol (mmol/l) 0,01 (-0.02 to -0.03) Effects of metformin on glycaemia and lipids: data from a meta-analysis. These data are from a meta-analysis of 41 studies of at least 6 weeks’ duration providing data on glycaemia, lipids and/or blood pressure in patients treated with metformin. Metformin treatment was associated with significant reductions in HbA1C, triglycerides, total cholesterol and LDL-cholesterol. HDL-cholesterol was unaffected. Metformin also did not affect systolic blood pressure (mean change mmHg [95% CI to 0.82] or diastolic blood pressure (mean change [95% CI to -0.21]). Wulffele MG, Kooy A, de Zeeuw D, Stehouwer CD, Gansevoort RT. The effect of metformin on blood pressure, plasma cholesterol and triglycerides in type 2 diabetes mellitus: a systematic review. J Intern Med 2004;256:1-14. Wulffele MG et al. J Intern Med 2004;256:1-14.")
9
Účinek metforminu na hladiny PAI-1
PAI-1 (AU/mL) Effects of metformin on levels of PAI-1 Plasminogen activator inhibitor-1 (PAI-1) is the endogenous inhibitor of tissue plasminogen activator (tPA), the two key components of the fibrinolytic system. Normally, the activities of PAI-1 and tPA are in balance. Increased levels of PAI-1 indicate depressed fibrinolysis and increased risk of an occlusive atherothrombotic event. Measurement of PAI-1 was included in a 12-week, randomised, double-blind crossover study in 27 type 2 diabetic patients. PAI-1 levels were reduced significantly following metformin treatment, compared with placebo. Nagi DK, Yudkin JS. Effects of metformin on insulin resistance, risk factors for cardiovascular disease, and plasminogen activator inhibitor in NIDDM subjects. A study of two ethnic groups. Diabetes Care 1993;16:621-9 Nagi DK, Yudkin JS. Diabetes Care 1993;16:621-9
 Effects of metformin on levels of PAI-1. Plasminogen activator inhibitor-1 (PAI-1) is the endogenous inhibitor of tissue plasminogen activator (tPA), the two key components of the fibrinolytic system. Normally, the activities of PAI-1 and tPA are in balance. Increased levels of PAI-1 indicate depressed fibrinolysis and increased risk of an occlusive atherothrombotic event. Measurement of PAI-1 was included in a 12-week, randomised, double-blind crossover study in 27 type 2 diabetic patients. PAI-1 levels were reduced significantly following metformin treatment, compared with placebo. Nagi DK, Yudkin JS. Effects of metformin on insulin resistance, risk factors for cardiovascular disease, and plasminogen activator inhibitor in NIDDM subjects. A study of two ethnic groups. Diabetes Care 1993;16: Nagi DK, Yudkin JS. Diabetes Care 1993;16:")
10
Vliv léčby metforminem na aktivitu faktoru XIII u osob s DM 2 typu
Factor XIII activity (units/mL) * Factor XIII activity in type 2 diabetic patients following metformin treatment Blood samples from 39 patients taking part in a separate evaluation of metformin were analysed. Patients randomised to double-blind metformin received 1500 mg/day for 3 weeks, after which the dose was increased to 3000 mg for a further 9 weeks. Metformin reduced Factor XIII activity dose-dependently. A global statistical analysis (ANCOVA) of these data, plus data on circulating Factor XIII A and B subunits, showed that the effect of metformin was significant (p=0.01). The magnitudes of the effects of metformin on the A and B subunits of Factor XIII, not shown here for clarity, were similar to the effects described above. This study adds reduced activity of Factor XIII to the potentially anti-atherothrombotic actions of metformin. Standeven KF, Ariens RA, Whitaker P, Ashcroft AE, Weisel JW, Grant PJ. The effect of dimethylbiguanide on thrombin activity, FXIII activation, fibrin polymerization, and fibrin clot formation. Diabetes 2002;51:189-97 * Placebo Metformin 1500 mg/den Metformin 3000 mg/den *p=0.01 vs placebo Standeven KF et al. Diabetes 2002;51:189-97
 * Factor XIII activity in type 2 diabetic patients following metformin treatment. Blood samples from 39 patients taking part in a separate evaluation of metformin were analysed. Patients randomised to double-blind metformin received 1500 mg/day for 3 weeks, after which the dose was increased to 3000 mg for a further 9 weeks. Metformin reduced Factor XIII activity dose-dependently. A global statistical analysis (ANCOVA) of these data, plus data on circulating Factor XIII A and B subunits, showed that the effect of metformin was significant (p=0.01). The magnitudes of the effects of metformin on the A and B subunits of Factor XIII, not shown here for clarity, were similar to the effects described above. This study adds reduced activity of Factor XIII to the potentially anti-atherothrombotic actions of metformin. Standeven KF, Ariens RA, Whitaker P, Ashcroft AE, Weisel JW, Grant PJ. The effect of dimethylbiguanide on thrombin activity, FXIII activation, fibrin polymerization, and fibrin clot formation. Diabetes 2002;51: * Placebo. Metformin mg/den. Metformin mg/den. *p=0.01 vs placebo. Standeven KF et al. Diabetes 2002;51:")
11
Vliv léčby metforminem na aktivitu faktoru VII u osob s DM 2 typu
Mean change from baseline in Factor VII antigen (%) Factor VII levels in type 2 diabetic patients following metformin treatment Factor VII plays an important role in the coagulation cascade, and elevated activity of Factor VII has been associated with an increased risk of mortality from myocardial infarction. The study described above was conducted in 44 type 2 diabetic patients treated with metformin or placebo for 6 months. Metformin treatment was associated with a significant (p=0.02), dose-related reduction in Factor VII antigen levels. Grant PJ. Metformin reduces circulating factor VII concentrations in patients with type 2 diabetes mellitus. Thromb Haemost 1998;80:209-10 Grant PJ. Thromb Haemost 1998; 80:209-10
 Factor VII levels in type 2 diabetic patients following metformin treatment. Factor VII plays an important role in the coagulation cascade, and elevated activity of Factor VII has been associated with an increased risk of mortality from myocardial infarction. The study described above was conducted in 44 type 2 diabetic patients treated with metformin or placebo for 6 months. Metformin treatment was associated with a significant (p=0.02), dose-related reduction in Factor VII antigen levels. Grant PJ. Metformin reduces circulating factor VII concentrations in patients with type 2 diabetes mellitus. Thromb Haemost 1998;80: Grant PJ. Thromb Haemost 1998; 80:")
12
Další antiaterogenní účinky metforminu
Účinek Potenciální přínos Oxidace Apoptózy, oxidativního poškození pozdních produktů glykace zánětu, oxidačního stresu/apoptózy exprese adhezních molekul na povrchu buněk endotelu Aterogeneze aktivace monocytů → makrofágy vychytávání lipidů makrofágy Other anti–atherogenic actions of metformin Considerable clinical and experimental evidence supports a range of other potential anti-atherogenic mechanisms of metformin, in addition to the effects on classical cardiovascular risk factors described above. Some of these, for example reduction of glycoxidation by removal of advanced glycation end-products, are independent of insulin. These additional potentially beneficial effects suggest that metformin may reduce cardiovascular risk to a greater extent than predicted by risk engines, which only use classical cardiovascular risk factors in their algorithms. Kurukulasuriya R, Banerji MA, Chaiken R, Lebovitz H. Selective decrease in visceral fat is associated with weight loss during metformin treatment in African Americans with type 2 diabetes. Diabetes 1999;48 Suppl:A315 Beisswenger P, Ruggiero-Lopez D. Metformin inhibition of glycation processes. Diabetes Metab 2003;29:6S95-103 Pavlović D, Kocić R, Kocić G et al. Effect of four-week metformin treatment on plasma and erythrocyte antioxidative defense enzymes in newly diagnosed obese patients with type 2 diabetes. Diabetes Obes Metab 2000;2:251-6 Mamputu JC, Wiernsperger NF, Renier G. Antiatherogenic properties of metformin: the experimental evidence. Diabetes Metab 2003;29:6S71-6 Wiernsperger NF, Bouskela E. Microcirculation in insulin resistance and diabetes: more than just a complication. Diabetes Metab 2003;29:6S77-87 Kurukulasuriya R et al. Diabetes 1999;48 Suppl:A315; Beisswenger P et al. Diabetes Metab 2003;29: 6S95-103; Pavlović D et al. Diabetes Obes Metab 2000;2:251-6; Mamputu JC et al. Diabetes Metab 2003;29:6S71-6. Wiernsperger NF et al. Diabetes Metab 2003;29:6S77-87

13
Metabolické účinky aktivace AMP kinázy
Fyzická aktivita Hypoxie/ischémie Tr-172 Inaktivní poměru AMP/ATP AMPK vazba AMP na AMPK Aktivní fosforylace treoninu-172 působením LKB1 metformin LKB1 P Aktivace AMPK Tr-172 AMP AMPK procesů tvorby a výdeje energie procesů spjatých s tvorbou zásob

14
2) Ve vztahu k buněčnému růstu?
Aktivace AMP- kinázy 1) Ve vztahu k diabetu výdej glukózy játry vychytávání glukózy tkáněmi udržuje senzitivitu tkání k inzulínu Snižuje hladinu glykémie 2) Ve vztahu k buněčnému růstu? antianabolická/prokatabolická úloha mediátor přirozených supresorů kancerogeneze zpomaluje/zastavuje aberantní buněčný růst
 Ve vztahu k diabetu. výdej glukózy játry. vychytávání glukózy tkáněmi. udržuje senzitivitu tkání k inzulínu. Snižuje hladinu glykémie. 2) Ve vztahu k buněčnému růstu antianabolická/prokatabolická úloha. mediátor přirozených supresorů kancerogeneze. zpomaluje/zastavuje aberantní buněčný růst.")
15
Uživatelé metforminu mají nižší riziko vzniku rakoviny Libby G, Diabetes Care,Volume 32, September 2009 Podíl osob bez nádorového onemocnění

16
Přehled studií vztahu metforminu a kancerogeneze
Počet pacientů Riziko incidence nádorů HAZARD RATIO (95% CI) Libby G. 4085 v.4085 UŽIVATELÉ METFORMINU 0,63 0,53-0,75 Bowker 12 272 UŽIVATELÉ SULFONYLUREY 1,3 UŽIVATELÉ INZULÍNU ,9 1,1-1,6 1,5-2,4 Monami 195 v.195 UŽIVATELÉ METFORMINU 0,28 0,13-0,57 Li Ca pankreatu 350 osob s DM 2.typu UŽIVATELÉ METFORMINU 0,38 0,22-0,69 Jiralespong Karcinom prsu 68 v.87 UŽIVATELKY METFORMINU 24% NE-UŽIVATELKY METFORMINU 8% KOMPLETNÍ REMISE
 Libby G v UŽIVATELÉ METFORMINU 0,63. 0,53-0,75. Bowker UŽIVATELÉ SULFONYLUREY 1,3 UŽIVATELÉ INZULÍNU 1,9. 1,1-1,6. 1,5-2,4. Monami. 195 v.195. UŽIVATELÉ METFORMINU 0,28. 0,13-0,57. Li. Ca pankreatu. 350 osob s DM 2.typu. UŽIVATELÉ METFORMINU 0,38. 0,22-0,69. Jiralespong. Karcinom prsu. 68 v.87. UŽIVATELKY METFORMINU 24% NE-UŽIVATELKY METFORMINU 8% KOMPLETNÍ REMISE.")
17
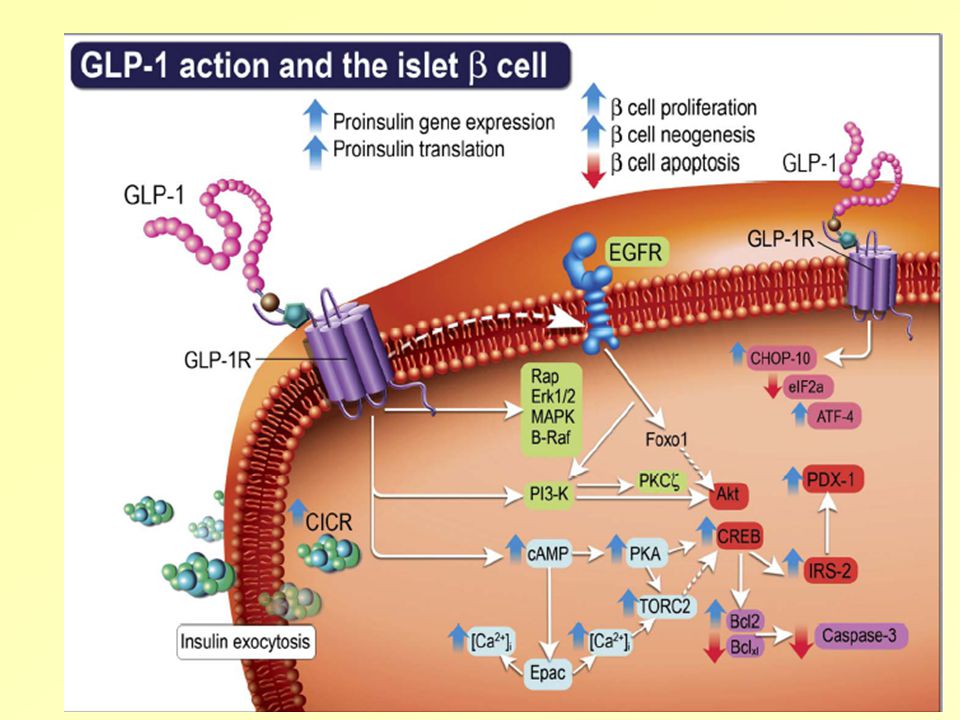
Účinky agonistů GLP-1 receptoru v lidské fyziologii
Pankreas Mozek Insulinové sekrece (na glukóze-závislé) a senzitivity buněk příjem stravy* játra výdej glukózy Syntézy inzulínu Liraglutide has multiple direct effects on human physiology 1. Pancreas and Liver GLP-1 has a direct functional effect on pancreatic cells, influencing secretions from alpha-, beta- and delta- cells. One of its most important effects is to increase insulin secretion. Importantly, however, its insulinotropic action is glucose dependent. Consequently, GLP-1 has the capacity to lower blood glucose while protecting against hypoglycaemia. GLP-1 also regulates glucagon secretion, partly via an increase in somatostatin secretion, and partly via a direct effect on the alpha-cell. This reduction in glucagon secretion serves to decrease hepatic glucose output. 2. GLP-1 stimulates -cell regeneration and mass in animal models Studies have demonstrated that GLP-1 plays an important role in maintaining -cells. In animal studies, GLP-1 increases -cell mass through the stimulation of -cell neogenesis, growth and proliferation. Proliferation results from differentiation and division of existing -cells, while neogenesis occurs through differentiation of insulin-secreting cells from precursor cells in the pancreatic ductal epithelium (Bulotta et al, 2002). Additionally, a study using freshly isolated human islets reported a reduction in the number of apoptotic -cells following 5 days of in vitro treatment with GLP-1 (Farilla et al, 2003). These observations of increased -cell mass and decreased apoptosis are of particular interest in the treatment of type 2 diabetes as progressive -cell dysfunction is one of the main pathophysiologies of the disease. 3. GLP-1: effects on the gastrointestinal, cardiac and central nervous systems The net effect of GLP-1’s action on the gastrointestinal system is to delay absorption of food. This is caused by several means, including decreased gastric emptying and acid secretion. For example, the infusion of GLP-1 to generate plasma levels similar to those normally observed following meals delays gastric emptying (Wettergren et al, 1993). Combined, these gastrointestinal effects serve to flatten the meal-related increase in glucose. This may be important in the management of type 2 diabetes because elevated postprandial glucose excursions are a key feature of type 2 diabetes. Reducing this excursion should therefore be an aim of diabetes treatment. Prolonged presence of food in the stomach through delayed gastric emptying may also reduce food intake by increasing the feeling of satiety. Additionally, GLP-1 receptors are present in several areas in the brain. The receptors in the brainstem (area postrema and subfornical organ) are believed to be involved in inducing feelings of satiety, regardless of the presence of food in the gastric system. This action therefore provides another means for decreasing food intake. Recently, GLP-1 has also been shown to improve spatial and associative learning following its intracerebroventricular infusion in the rat (During et al, 2003). Furthermore, studies have shown that GLP-1 can protect CNS cells against apoptosis (in vitro, Perry et al 2002), and reduce amyloid levels (in vivo, Perry et al 2003). GLP-1 has also been associated with cardiovascular function in animal and human studies. Specifically, studies have shown that use of GLP-1 or recombinant GLP-1 can protect myocardium in ischaemic conditions (Bose et al 2005, Kavianipour et al 2003), improve myocardial function (Thrainsdottir et al 2004, Nikolaidis, Mankad et al 2004), improve endothelial function (Nystrom et al 2004), and relax arteries (Nystrom et al 2005). References Wettergren et al. Dig Dis Sci 1993;38:665–73. Kieffer, et al. Endocr Rev 1999;20:876–913. During et al. Nat Med 2003;9:1173–9. Flint et al. J Clin Invest 1998;101:515–20. Perry et al. J Pharmacol Exp Ther 2002;302:881–8. Perry et al. J Neurosci Res 2003;72:603–12. Bose et al. Diabetes 2005;54:146–51. Kavianipour et al. Peptides 2003;24:569–78. Thrainsdottir et al. Diab Vasc Dis Res 2004;1:40–3. Nikolaidis et al. Circulation 2004;109:962–5. Nystrom et al. Am J Physiol Endocrinol Metab 2004;287:E1209–15. Nystrom et al. Regul Pept 2005;125:173–7. Drucker et al. Proc Natl Acad Sci USA 1987;84:3434–8. Ørskov et al. Endocrinology 1988;123:2009–13. Bulotta et al. J Mol Endocrinol 2002;29:347–60. Farilla et al. Endocrinology 2003;144:5149–58. Sekrece glukagonu (na glukóze závisle) GI trakt Motilita – zejména vyprazdňování žaludku *in animal studies 17
 a senzitivity buněk. příjem stravy* játra. výdej glukózy. Syntézy inzulínu. Liraglutide has multiple direct effects on human physiology. 1. Pancreas and Liver. GLP-1 has a direct functional effect on pancreatic cells, influencing secretions from alpha-, beta- and delta- cells. One of its most important effects is to increase insulin secretion. Importantly, however, its insulinotropic action is glucose dependent. Consequently, GLP-1 has the capacity to lower blood glucose while protecting against hypoglycaemia. GLP-1 also regulates glucagon secretion, partly via an increase in somatostatin secretion, and partly via a direct effect on the alpha-cell. This reduction in glucagon secretion serves to decrease hepatic glucose output. 2. GLP-1 stimulates -cell regeneration and mass in animal models. Studies have demonstrated that GLP-1 plays an important role in maintaining -cells. In animal studies, GLP-1 increases -cell mass through the stimulation of -cell neogenesis, growth and proliferation. Proliferation results from differentiation and division of existing -cells, while neogenesis occurs through differentiation of insulin-secreting cells from precursor cells in the pancreatic ductal epithelium (Bulotta et al, 2002). Additionally, a study using freshly isolated human islets reported a reduction in the number of apoptotic -cells following 5 days of in vitro treatment with GLP-1 (Farilla et al, 2003). These observations of increased -cell mass and decreased apoptosis are of particular interest in the treatment of type 2 diabetes as progressive -cell dysfunction is one of the main pathophysiologies of the disease. 3. GLP-1: effects on the gastrointestinal, cardiac and central nervous systems. The net effect of GLP-1’s action on the gastrointestinal system is to delay absorption of food. This is caused by several means, including decreased gastric emptying and acid secretion. For example, the infusion of GLP-1 to generate plasma levels similar to those normally observed following meals delays gastric emptying (Wettergren et al, 1993). Combined, these gastrointestinal effects serve to flatten the meal-related increase in glucose. This may be important in the management of type 2 diabetes because elevated postprandial glucose excursions are a key feature of type 2 diabetes. Reducing this excursion should therefore be an aim of diabetes treatment. Prolonged presence of food in the stomach through delayed gastric emptying may also reduce food intake by increasing the feeling of satiety. Additionally, GLP-1 receptors are present in several areas in the brain. The receptors in the brainstem (area postrema and subfornical organ) are believed to be involved in inducing feelings of satiety, regardless of the presence of food in the gastric system. This action therefore provides another means for decreasing food intake. Recently, GLP-1 has also been shown to improve spatial and associative learning following its intracerebroventricular infusion in the rat (During et al, 2003). Furthermore, studies have shown that GLP-1 can protect CNS cells against apoptosis (in vitro, Perry et al 2002), and reduce amyloid levels (in vivo, Perry et al 2003). GLP-1 has also been associated with cardiovascular function in animal and human studies. Specifically, studies have shown that use of GLP-1 or recombinant GLP-1 can protect myocardium in ischaemic conditions (Bose et al 2005, Kavianipour et al 2003), improve myocardial function (Thrainsdottir et al 2004, Nikolaidis, Mankad et al 2004), improve endothelial function (Nystrom et al 2004), and relax arteries (Nystrom et al 2005). References. Wettergren et al. Dig Dis Sci 1993;38:665–73. Kieffer, et al. Endocr Rev 1999;20:876–913. During et al. Nat Med 2003;9:1173–9. Flint et al. J Clin Invest 1998;101:515–20. Perry et al. J Pharmacol Exp Ther 2002;302:881–8. Perry et al. J Neurosci Res 2003;72:603–12. Bose et al. Diabetes 2005;54:146–51. Kavianipour et al. Peptides 2003;24:569–78. Thrainsdottir et al. Diab Vasc Dis Res 2004;1:40–3. Nikolaidis et al. Circulation 2004;109:962–5. Nystrom et al. Am J Physiol Endocrinol Metab 2004;287:E1209–15. Nystrom et al. Regul Pept 2005;125:173–7. Drucker et al. Proc Natl Acad Sci USA 1987;84:3434–8. Ørskov et al. Endocrinology 1988;123:2009–13. Bulotta et al. J Mol Endocrinol 2002;29:347–60. Farilla et al. Endocrinology 2003;144:5149–58. Sekrece glukagonu (na glukóze závisle) GI trakt. Motilita – zejména vyprazdňování žaludku. *in animal studies. 17.")
19
Nativní GLP-1 je rychle degradován prostřednictvím DPP-4
7 36 9 -NH2 His Ala Glu Gly Thr Phe Ser Asp Val Tyr Leu Gln Lys Ile Trp Plasma T½ =1-2 minutes (i.v.) MCR = 5-10 l/min Těsný histologický vztah struktur DPP-4 a GLP-1 pozitivních v tenkém střevě DPP-4=dipeptidyl peptidase 4 Hansen L et al, Endocrinology 1999; 140: MCR=metabolic clearance rate. Vilsbøll T et al. J Clin Endocrinol Metab. 2003;88:220–224.
 MCR = 5-10 l/min. Těsný histologický vztah struktur DPP-4 a GLP-1 pozitivních v tenkém střevě. DPP-4=dipeptidyl peptidase 4. Hansen L et al, Endocrinology 1999; 140: MCR=metabolic clearance rate. Vilsbøll T et al. J Clin Endocrinol Metab. 2003;88:220–224.")
20
Struktura dipeptidyl peptidázy - 4

21
Aktivní místo dipeptidyl peptidázy- 4

22
Léčebné modality odvozené od účinku inkretinů
Slide No 22 Léčebné modality odvozené od účinku inkretinů The family of incretin-based therapies Incretin-based therapies can be broadly divided into: DPP-4 inhibitors (i.e. sitagliptin, vildagliptin) GLP-1 receptor agonists (Exenatide, lirgalutide) Within this second category however, the GLP-1R agonists can be classed as either: Exendin-based therapies (exenatide, exenatide LAR) which have ~50% sequence identity to human GLP-1 Human GLP-1 analogues (liraglutide) which have share a much higher percentage of amino acids with human GLP-1 (97%) Humánní GLP-1 analoga, např. Liraglutid, albiglutid Od exendinu odvozená léčiva, exenatid, exenatid LAR Agonisté GLP-1 receptoru DPP-4 inhibitory, např. sitagliptin, vildagliptin saxagliptin Léčiva působící přes změny hladin inkretinů 22
 GLP-1 receptor agonists (Exenatide, lirgalutide) Within this second category however, the GLP-1R agonists can be classed as either: Exendin-based therapies (exenatide, exenatide LAR) which have ~50% sequence identity to human GLP-1. Human GLP-1 analogues (liraglutide) which have share a much higher percentage of amino acids with human GLP-1 (97%) Humánní GLP-1. analoga, např. Liraglutid, albiglutid. Od exendinu odvozená. léčiva, exenatid, exenatid LAR. Agonisté. GLP-1 receptoru. DPP-4 inhibitory, např. sitagliptin, vildagliptin. saxagliptin. Léčiva působící přes změny hladin inkretinů. 22.")
23
Mechanismus účinku inhibitorů DPP - 4

24
DPP-4 inhibitor (vildagliptin) dose
Koncentrace mimetik je vyšší než koncentrace GLP-1 navozená podáním DPP-4 inhibitoru GLP-1 levels after 7 days’ liraglutide 6 µg/kg OD* (n=13) GLP-1 levels after 28 days’ vildagliptin 100 mg BD (n=9) 120 120 Liraglutide dose 90 90 GLP-1 (pmol/L) DPP-4 inhibitor (vildagliptin) dose 60 60 30 30 Concentration of active liraglutide is higher than GLP-1 concentration with a DPP-4 inhibitor These studies show that the level of the GLP-1 receptor agonist, liraglutide, are higher than that achieved with a DPP-4 inhibitor such as vildagliptin. The pharmacological levels of GLP-1R agonist achieved with liraglutide result in additional clinical benefits for example weight loss, as compared with DPP-4 inhibitors, which are weight neutral. References Degn et al. Diabetes 2004;53:1187–94. Mari et al. J Clin Endocrinol Metab 2005;90:4888–94 8 12 16 20 24 8 12 16 20 24 Time (h) Time (h) *GLP-1 levels for liraglutide calculated as 1.5% free liraglutide Degn et al. Diabetes 2004;53:1187–94. Mari et al. J Clin Endocrinol Metab 2005;90:4888–94 24
 GLP-1 levels after 28 days’ vildagliptin 100 mg BD (n=9) Liraglutide dose GLP-1 (pmol/L) DPP-4 inhibitor (vildagliptin) dose Concentration of active liraglutide is higher than GLP-1 concentration with a DPP-4 inhibitor. These studies show that the level of the GLP-1 receptor agonist, liraglutide, are higher than that achieved with a DPP-4 inhibitor such as vildagliptin. The pharmacological levels of GLP-1R agonist achieved with liraglutide result in additional clinical benefits for example weight loss, as compared with DPP-4 inhibitors, which are weight neutral. References. Degn et al. Diabetes 2004;53:1187–94. Mari et al. J Clin Endocrinol Metab 2005;90:4888– Time (h) Time (h) *GLP-1 levels for liraglutide calculated as 1.5% free liraglutide. Degn et al. Diabetes 2004;53:1187–94. Mari et al. J Clin Endocrinol Metab 2005;90:4888–")
25
Farmakodynamické vlastnosti sitagliptinu

26
Synergický účinek sitagliptinu a metforminu
Terapie počet geometrický průměr plochy poměr ve vztahu k placebu 95% CI‡ statistická významnost aktivní GLP-1 (pM) SITA MF 16 16.37 14.81 1.95 1.76 (1.58, 2.40) (1.43, 2.17) <0.001 SITA + MF PBO 15 34.68 8.41 4.12 (3.35, 5.08) celkový GLP-1 (pM) 12.43 32.14 0.70 1.81 (0.58, 0.85) (1.49, 2.20) 27.82 17.77 1.57 (1.29, 1.90)
 SITA. MF (1.58, 2.40) (1.43, 2.17) < SITA + MF. PBO (3.35, 5.08) celkový GLP-1 (pM) (0.58, 0.85) (1.49, 2.20) (1.29, 1.90)")
27
Efekt iniciální kombinace sitagliptinu a metforminu u nemocných s DM 2
Efekt iniciální kombinace sitagliptinu a metforminu u nemocných s DM 2. typu ( HbA1c )
")
28
Efekt iniciální kombinace sitagliptinu a metforminu u nemocných s DM 2
Efekt iniciální kombinace sitagliptinu a metforminu u nemocných s DM 2. typu ( HbA1c )
")
29
Analýza bezpečnosti a tolerance sitagliptinu
12 studií fáze IIb a III Sita (n=3145) PBO (n=2742) s léčivem spojené nežádoucí příhody 12,9% 17,7% Závažné nežádoucí příhody 6,7% 6,8% úmrtí 11 16 Kardiální nežádoucí příhody 1,2% 1,5% Ischemické nežádoucí příhody 2,0% 2,3% pankreatitidy 0,1% 0% Wiliams-Herman D., et al. EASD 2008
 PBO (n=2742) s léčivem spojené nežádoucí příhody. 12,9% 17,7% Závažné nežádoucí příhody. 6,7% 6,8% úmrtí Kardiální nežádoucí příhody. 1,2% 1,5% Ischemické nežádoucí příhody. 2,0% 2,3% pankreatitidy. 0,1% 0% Wiliams-Herman D., et al. EASD")
30
Nežádoucí účinky při léčbě sitagliptinem
Frekvence přerušení léčby sitagliptinem byla podobná jako u placeba Incidence hypoglykemií při léčbě sitagliptinem byla podobná jakou u placeba (1.2% vs 0.9%) Incidence GIT nežádoucích příhod při léčbě sitagliptinem byla podobná ve srovnání s placebem: bolesti břicha (2.3%, 2.1%) nausea (1.4%, 0.6%) průjem (3.0%, 2.3%) zvracení (0.8%, 0.9%) JANUVIA™† (sitagliptin): Adverse Reactions This slide provides a brief overview of the adverse reaction profile for JANUVIA. Overall, JANUVIA was generally well tolerated in controlled clinical studies as both monotherapy and combination therapy. Discontinuation of therapy as both monotherapy and combination therapy due to clinical adverse experiences was similar to placebo. The overall incidence of hypoglycemia in patients treated with JANUVIA was similar to that of placebo (1.2% vs 0.9%, respectively). The incidence of selected gastrointestinal (GI) adverse reactions in patients treated with JANUVIA was as follows: abdominal pain JANUVIA 100 mg, 2.3%; placebo, 2.1%), nausea (1.4%, 0.6%), diarrhea (3.0%, 2.3%), and vomiting (0.8%, 0.9%). The following additional adverse reactions have been identified during postmarketing use of JANUVIA. Because the reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure: Hypersensitivity reactions, including anaphylaxis, angioedema, rash, and urticaria; upper respiratory tract infection; nasopharyngitis. Purpose: To review the adverse events profile for JANUVIA. Takeaway: JANUVIA has a low risk of hypoglycemia and is generally well tolerated. In monotherapy and combination therapy with JANUVIA, discontinuation of therapy due to clinical adverse experiences was similar to placebo. 47 †Trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA Reference 1. Data on file.
 Incidence GIT nežádoucích příhod při léčbě sitagliptinem byla podobná ve srovnání s placebem: bolesti břicha (2.3%, 2.1%) nausea (1.4%, 0.6%) průjem (3.0%, 2.3%) zvracení (0.8%, 0.9%) JANUVIA™† (sitagliptin): Adverse Reactions. This slide provides a brief overview of the adverse reaction profile for JANUVIA. Overall, JANUVIA was generally well tolerated in controlled clinical studies as both monotherapy and combination therapy. Discontinuation of therapy as both monotherapy and combination therapy due to clinical adverse experiences was similar to placebo. The overall incidence of hypoglycemia in patients treated with JANUVIA was similar to that of placebo (1.2% vs 0.9%, respectively). The incidence of selected gastrointestinal (GI) adverse reactions in patients treated with JANUVIA was as follows: abdominal pain JANUVIA 100 mg, 2.3%; placebo, 2.1%), nausea (1.4%, 0.6%), diarrhea (3.0%, 2.3%), and vomiting (0.8%, 0.9%). The following additional adverse reactions have been identified during postmarketing use of JANUVIA. Because the reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure: Hypersensitivity reactions, including anaphylaxis, angioedema, rash, and urticaria; upper respiratory tract infection; nasopharyngitis. Purpose: To review the adverse events profile for JANUVIA. Takeaway: JANUVIA has a low risk of hypoglycemia and is generally well tolerated. In monotherapy and combination therapy with JANUVIA, discontinuation of therapy due to clinical adverse experiences was similar to placebo. 47. †Trademark of Merck & Co., Inc., Whitehouse Station, NJ, USA. Reference. 1. Data on file.")
31
Nežádoucí účinky s incidencí ≥ 2% Analýza 12 studií
Nežádoucí účinek Sitagliptin 100 mg N = 3415 Neexponované osoby N = 2724 Rozdíl mezi sitagliptinem a ne-exponovanými % (95% CI) n (%) zácpa 79 (2.3) 47 (1.7) 0.6 (-0.1, 1.3) průjem 170 (5.0) 144 (5.3) -0.3 (-1.4, 0.8) dyspepsie 70 (2.0) 40 (1.5) 0.6 (-0.1, 1.2) nausea 85 (2.5) 70 (2.6) -0.1 (-0.9, 0.7) periferní edém 62 (1.8) 54 (2.0) -0.2 (-0.9, 0.5) bronchitis 135 (4.0) 83 (3.0) 0.9 (-0.0, 1.8) gastroenteritis 68 (2.0) 48 (1.8) 0.2 (-0.5, 0.9) influenza 145 (4.2) 127 (4.7) -0.4 (-1.5, 0.6) nasofaryngitis 244 (7.1) 162 (5.9) 1.2 (-0.1, 2.4) sinusitis 80 (2.3) 60 (2.2) 0.1 (-0.6, 0.9) All AEs with an incidence (proportion of patients with at least 1 event) >/=2% in either group Regardless of causality Majority of differences are small (<1%) Nasopharyngitis is the only AE with a difference in incidence >1% and higher in the sitagliptin group
 n (%) zácpa. 79 (2.3) 47 (1.7) 0.6 (-0.1, 1.3) průjem. 170 (5.0) 144 (5.3) -0.3 (-1.4, 0.8) dyspepsie. 70 (2.0) 40 (1.5) 0.6 (-0.1, 1.2) nausea. 85 (2.5) 70 (2.6) -0.1 (-0.9, 0.7) periferní edém. 62 (1.8) 54 (2.0) -0.2 (-0.9, 0.5) bronchitis. 135 (4.0) 83 (3.0) 0.9 (-0.0, 1.8) gastroenteritis. 68 (2.0) 48 (1.8) 0.2 (-0.5, 0.9) influenza. 145 (4.2) 127 (4.7) -0.4 (-1.5, 0.6) nasofaryngitis. 244 (7.1) 162 (5.9) 1.2 (-0.1, 2.4) sinusitis. 80 (2.3) 60 (2.2) 0.1 (-0.6, 0.9) All AEs with an incidence (proportion of patients with at least 1 event) >/=2% in either group. Regardless of causality. Majority of differences are small (<1%) Nasopharyngitis is the only AE with a difference in incidence >1% and higher in the sitagliptin group.")
32
Srovnání struktury humánního GLP-1 a jeho analoga liraglutidu
Nativní humánní GLP-1 pomalá absorpce z podkoží Rezistentní vůči DPP-4 dlouhý plasmatický poločas (T½=13 h) vazba na albumin tvorba heptamerů mastná kys. (palmitoyl) His Ala Thr Ser Phe Glu Gly Asp Val Tyr Leu Gln Lys Ile Trp Arg 7 9 36 Liraglutid T½=1.5–2.1 min Enzymatická degradace DPP-4 7 36 9 Lys His Ala Thr Ser Phe Glu Gly Asp Val Tyr Leu Gln Ile Trp Arg Liraglutide is a once-daily human GLP-1 analogue In creating liraglutide, two modifications to the amino acid sequence of GLP-1 are made: a fatty acid is acylated to lysine at position 26 and the lysine at position 34 is replaced with arginine. These modifications result in increased self-association (which slows absorption from the subcutaneous depot), albumin binding and reduced susceptibility to DPP-IV, which combine to prolong its plasma half-life, protracting its action. Thus, the problem of the short half-life, which is the major clinical drawback of native GLP-1, is overcome. For comparison, the plasma half-life of exenatide is 4 to 6 hours (reviewed in Drucker and Nauck, 2006) Reference Knudsen et al. J Med Chem 2000;43:1664–69 Degn et al. Diabetes 2004;53:1187–94
 vazba na albumin. tvorba heptamerů. mastná kys. (palmitoyl) His. Ala. Thr. Ser. Phe. Glu. Gly. Asp. Val. Tyr. Leu. Gln. Lys. Ile. Trp. Arg Liraglutid. T½=1.5–2.1 min. Enzymatická degradace DPP Lys. His. Ala. Thr. Ser. Phe. Glu. Gly. Asp. Val. Tyr. Leu. Gln. Ile. Trp. Arg. Liraglutide is a once-daily human GLP-1 analogue. In creating liraglutide, two modifications to the amino acid sequence of GLP-1 are made: a fatty acid is acylated to lysine at position 26 and the lysine at position 34 is replaced with arginine. These modifications result in increased self-association (which slows absorption from the subcutaneous depot), albumin binding and reduced susceptibility to DPP-IV, which combine to prolong its plasma half-life, protracting its action. Thus, the problem of the short half-life, which is the major clinical drawback of native GLP-1, is overcome. For comparison, the plasma half-life of exenatide is 4 to 6 hours (reviewed in Drucker and Nauck, 2006) Reference. Knudsen et al. J Med Chem 2000;43:1664–69. Degn et al. Diabetes 2004;53:1187–94.")
33
Hladiny liraglutidu a exenatidu v ustáleném stavu
exenatide BD T½ 2.4 h pM liraglutide OD T½ 13 h nM 28 100 50 24 80 40 20 60 30 16 Normalised concentration (%) Absolute concentration 40 20 12 20 8 10 Steady state levels of GLP-1 with liraglutide and exenatide The aim of this modeling study was to develop a pharmacokinetic model on available data on liraglutide and exenatide in man, and thereby compare their pharmacokinetic properties. A population-based modelling approach was taken to describe the time course of liraglutide concentrations and its inter-and intrasubject variability using NONMEM V. The absorption of liraglutide following subcutaneous (sc) administration was slow, reaching a maximum 9–12 hours post-dosing. Liraglutide concentrations were adequately described by a one-compartment model with saturable, dose-dependent absorption and first-order elimination. The PK of liraglutide was found to be dose-linear except at the lowest dose, at which exposure was subproportional. The Figure shows the PK profiles at steady state for 20 μg/kg liraglutide once daily sc (solid line) and for 10 μg/kg exenatide twice daily sc (dashed line). Liraglutide steady state was reached on day 3. Reference Jonker et al. Diabetes 56(Suppl. 1):A160 (Abstract 0605-P) 4.0 4.5 5.0 5.5 6.0 6.5 7.0 Time after first dose (days) Modelling of plasma concentration of active drug vs. maximal concentration at steady state achieved following clinically relevant doses OD or BD. Based on published exenatide data and modelled liraglutide data. Jonker et al. Diabetes 56(Suppl. 1):A160 33
 Absolute concentration Steady state levels of GLP-1 with liraglutide and exenatide. The aim of this modeling study was to develop a pharmacokinetic model on available data on liraglutide and exenatide in man, and thereby compare their pharmacokinetic properties. A population-based modelling approach was taken to describe the time course of liraglutide concentrations and its inter-and intrasubject variability using NONMEM V. The absorption of liraglutide following subcutaneous (sc) administration was slow, reaching a maximum 9–12 hours post-dosing. Liraglutide concentrations were adequately described by a one-compartment model with saturable, dose-dependent absorption and first-order elimination. The PK of liraglutide was found to be dose-linear except at the lowest dose, at which exposure was subproportional. The Figure shows the PK profiles at steady state for 20 μg/kg liraglutide once daily sc (solid line) and for 10 μg/kg exenatide twice daily sc (dashed line). Liraglutide steady state was reached on day 3. Reference. Jonker et al. Diabetes 56(Suppl. 1):A160 (Abstract 0605-P) Time after first dose (days) Modelling of plasma concentration of active drug vs. maximal concentration at steady state achieved following clinically relevant doses OD or BD. Based on published exenatide data and modelled liraglutide data. Jonker et al. Diabetes 56(Suppl. 1):A")
34
Srovnání účinku liraglutidu a exenatidu na kompenzaci diabetu
Baseline 8.2% Baseline 8.1% Draft ICTR (27 August 2008): Table 11.3 (baseline values); table 11.4 p<0.0001 Both liraglutide and exenatide was combined with met and/or SU Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 34
: Table 11.3 (baseline values); table p< Both liraglutide and exenatide was combined with met and/or SU. Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 34.")
35
Liraglutid i exenatide dlouhodobě redukují tělesnou hmotnost
Time since randomisation (weeks) 4 8 12 16 20 26 -1 -2 Change in body weight (kg) -3 NS -4 EOT_14_2_extra_lbuj; Figure Figure requires 2SE values and p-values, if any -5 Liraglutide 1.8 mg OD Exenatide 10 μg BID Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 35
 Change in body weight (kg) -3. NS. -4. EOT_14_2_extra_lbuj; Figure Figure requires 2SE values and p-values, if any. -5. Liraglutide 1.8 mg OD. Exenatide 10 μg BID. Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 35.")
36
Srovnání incidence nausey liraglutid vs. exenatid
Proportion of subjects with nausea by week and treatment 20 Exenatide 10 μg BID Liraglutide 1.8 mg OD 16 18 14 Proportion of subjects (%) 10 12 8 6 4 Draft ICTR (27 August 2008): Figure 12.2; information about number of withdrawals in each treatment group due to nausea to be added 2 2 4 6 8 10 12 14 16 18 20 22 24 26 28 Time (weeks) Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 36
 Draft ICTR (27 August 2008): Figure 12.2; information about number of withdrawals in each treatment group due to nausea to be added Time (weeks) Blonde et al. Can J Diabetes 2008;32(Suppl): A107 (LEAD 6). 36.")
37
Účinek kombinací PAD (jejichž základem je metformin)
HbA1C (%) Vstupní hodnota Průměrná změna Metformin + glibenklamid1 8.8 –1.7 Metformin + glimepirid2 6.5 -0.7 Metformin + repaglinid3 8.5 -1.4 Metformin + pioglitazon4 9.8 -0.6 Metformin + rosiglitazon5 -0.8 Metformin + akarbosa6 8.3 Efficacy of co-administered combinations based on metformin Metformin is suitable for combination with any other oral antidiabetic agent. Clinical studies have shown that metformin reduced blood glucose effectively when combined with a sulfonylurea, a meglitinide, a thiazolidinedione, or an a-glucosidase inhibitor. DeFronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin dependent diabetes mellitus. N Engl J Med 1995;333:541-9 Charpentier G, Fleury F, Kabir M et al. Improved glycaemic control by addition of glimepiride to metformin monotherapy in type 2 diabetic patients. Diabet Med 2001;16:828-34 Moses R, Carter J, Slobodniuk R et al. Effect of repaglinide addition to metformin monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 1999;22:119-24 Einhorn D, Rendell M, Rosenzweig J et al. Pioglitazone hydrochloride in combination with metformin in the treatment of type 2 diabetes mellitus: A randomized, placebo-controlled study. Clin Ther 2000;22: Fonseca V, Rosenstock J, Patwardhan R et al. Effect of metformin and rosiglitazone combination therapy in patients with type 2 diabetes mellitus. JAMA 2000;283: Rosenstock J, Nadeau D, Brown A et al. Efficacy and safety of acarbose in metformin-treated patients with type 2 diabetes. Diabetes Care 1998;21: 1DeFronzo RA et al. N Engl J Med 1995;333:541-9; 2Charpentier G et al. Diabet Med 2001;16: Moses R et al. Diabetes Care 1999;22:119-24; 4Einhorn D et al. Clin Ther 2000;22: Fonseca V et al. JAMA 2000;283: ; 6Rosenstock J et al. Diabetes Care 1998;21:2050-5
 Vstupní hodnota. Průměrná změna. Metformin + glibenklamid –1.7. Metformin + glimepirid Metformin + repaglinid Metformin + pioglitazon Metformin + rosiglitazon Metformin + akarbosa Efficacy of co-administered combinations based on metformin. Metformin is suitable for combination with any other oral antidiabetic agent. Clinical studies have shown that metformin reduced blood glucose effectively when combined with a sulfonylurea, a meglitinide, a thiazolidinedione, or an a-glucosidase inhibitor. DeFronzo RA, Goodman AM. Efficacy of metformin in patients with non-insulin dependent diabetes mellitus. N Engl J Med 1995;333: Charpentier G, Fleury F, Kabir M et al. Improved glycaemic control by addition of glimepiride to metformin monotherapy in type 2 diabetic patients. Diabet Med 2001;16: Moses R, Carter J, Slobodniuk R et al. Effect of repaglinide addition to metformin monotherapy on glycemic control in patients with type 2 diabetes. Diabetes Care 1999;22: Einhorn D, Rendell M, Rosenzweig J et al. Pioglitazone hydrochloride in combination with metformin in the treatment of type 2 diabetes mellitus: A randomized, placebo-controlled study. Clin Ther 2000;22: Fonseca V, Rosenstock J, Patwardhan R et al. Effect of metformin and rosiglitazone combination therapy in patients with type 2 diabetes mellitus. JAMA 2000;283: Rosenstock J, Nadeau D, Brown A et al. Efficacy and safety of acarbose in metformin-treated patients with type 2 diabetes. Diabetes Care 1998;21: DeFronzo RA et al. N Engl J Med 1995;333:541-9; 2Charpentier G et al. Diabet Med 2001;16: Moses R et al. Diabetes Care 1999;22:119-24; 4Einhorn D et al. Clin Ther 2000;22: Fonseca V et al. JAMA 2000;283: ; 6Rosenstock J et al. Diabetes Care 1998;21:")
38
Roční procentuální četnost Intenzif. Inz. režim (n=38)
Srovnání rizika hypoglykémie při léčbě metforminem, deriváty SU a inzulínem analýza z UKPDS Roční procentuální četnost hypoglykémií 5 10 15 20 25 30 35 Diet (n=756) Metformin (n=290) Sulfonylurea (n=1418) Bazální insulin (n=1036) Intenzif. Inz. režim (n=38) jakákoli hypoglykémie významná hypoglykémie A recent analysis from the UKPDS confirms the low risk of hypoglycaemia with metformin Tolerability data from patients maintained on antidiabetic monotherapy for 6 years have recently been analysed and published as UKPDS 73. The annual rate of hypoglycaemia in patients receiving oral antidiabetic monotherapy or insulin-based regimens is shown on the slide. The frequency of any hypoglycaemic event was low in the diet and metformin groups, higher in the sulfonylurea group, and highest of all in the insulin groups. The annual percentage of substantive hypoglycaemia was low in patients randomised to diet or oral antidiabetic monotherapy, and higher in patients randomised to insulin. The 95% confidence intervals overlapped for the annual percentage rates in patients randomised to diet (0.1 [95% CI 0.1 to 0.2]) or metformin (0.3 [95% CI 0.1 to 1.1]), indicating no significant difference between them. These data are consistent with the large body of clinical experience which has shown that treatment with metformin is not associated with hypoglycaemia to a clinically significant extent. Wright AD et al. Hypoglycemia in Type 2 diabetic patients randomized to and maintained on monotherapy with diet, sulfonylurea, metformin, or insulin for 6 years from diagnosis: UKPDS73. J Diabetes Complications 2006;20: Substantive hypoglycaemia: patients temporarily incapacitated but not requiring help, incapacitated and required help, or required medical attention or glucagon injection. Wright AD et al. J Diabetes Complications 2006;20:
 Metformin (n=290) Sulfonylurea (n=1418) Bazální insulin (n=1036) Intenzif. Inz. režim (n=38) jakákoli hypoglykémie. významná hypoglykémie. A recent analysis from the UKPDS confirms the low risk of hypoglycaemia with metformin. Tolerability data from patients maintained on antidiabetic monotherapy for 6 years have recently been analysed and published as UKPDS 73. The annual rate of hypoglycaemia in patients receiving oral antidiabetic monotherapy or insulin-based regimens is shown on the slide. The frequency of any hypoglycaemic event was low in the diet and metformin groups, higher in the sulfonylurea group, and highest of all in the insulin groups. The annual percentage of substantive hypoglycaemia was low in patients randomised to diet or oral antidiabetic monotherapy, and higher in patients randomised to insulin. The 95% confidence intervals overlapped for the annual percentage rates in patients randomised to diet (0.1 [95% CI 0.1 to 0.2]) or metformin (0.3 [95% CI 0.1 to 1.1]), indicating no significant difference between them. These data are consistent with the large body of clinical experience which has shown that treatment with metformin is not associated with hypoglycaemia to a clinically significant extent. Wright AD et al. Hypoglycemia in Type 2 diabetic patients randomized to and maintained on monotherapy with diet, sulfonylurea, metformin, or insulin for 6 years from diagnosis: UKPDS73. J Diabetes Complications 2006;20: Substantive hypoglycaemia: patients temporarily incapacitated but not requiring help, incapacitated and required help, or required medical attention or glucagon injection. Wright AD et al. J Diabetes Complications 2006;20:")
41
Náhodně zařazeny k určité alternativě kombinace PAD
Design studie RECORD Náhodně zařazeny k určité alternativě kombinace PAD Osoby léčené monoterapií přidán rosiglitazon (pokračuje metformin) metformin přidána sulfonylurea (pokračuje metformin) přidán rosiglitazon (pokračuje sulfonylurea) sulfonylurea přidán metformin (pokračuje sulfonylurea)
 metformin. přidána sulfonylurea (pokračuje metformin) přidán rosiglitazon (pokračuje sulfonylurea) sulfonylurea. přidán metformin (pokračuje sulfonylurea)")
42
Úmrtí nebo hospitalizace z kardiovaskulárních příčin
Favorizuje rosiglitazon Favorizuje srovnávací terapii HR (95% CI) Primary analysis (ITT) 0.99 (0.85,1.16) Per protocol* 1.02 (0.85,1.21) Atherosclerotic events only 0.97 (0.82,1.14) původní metformin rosiglitazon versus SU 1.01 (0.81,1.26) původní SU rosiglitazon versus metformin 0.98 (0.79,1.21) 0.5 0.75 1.0 1.2 1.5 2.0 Hazard ratio (95% CI)
 Primary analysis (ITT) 0.99 (0.85,1.16) Per protocol* 1.02 (0.85,1.21) Atherosclerotic events only (0.82,1.14) původní metformin rosiglitazon versus SU (0.81,1.26) původní SU rosiglitazon versus metformin (0.79,1.21) Hazard ratio (95% CI)")
44
Při diagnóze: životospráva + metformin
1. pořadí: dobře ověřené léčebné modality životospráva + metformin + intenzif. inzulín. režim životospráva + metformin + bazální inzulín Při diagnóze: životospráva + metformin životospráva + metformin + Sulfonylureaa KROK KROK KROK 3 2.pořadí: méně ověřené léčebné modality životospráva + metformin + pioglitazon žádné hypoglykémie edémy/ srdeční selhání osteoporosa životospráva + metformin + pioglitazon + sulfonylureaa životospráva + metformin + GLP-1 agonista žádné hypoglykémie pokles hmotnosti nausea/zvracení životospráva + metformin bazální inzulín

Podobné prezentace