Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
UPV- umělá plícní ventilace
MUDr. V. Zvoníček

2
ARDS příčina akutní respirační selhání: tachypnoe, cyanosa, hypoxie
extrapulmonární: systémová infekce )sepse), tkáňová ischemie, nekrozy, trauma tkání pulmonární: pneumonie, aspirace, kontuze, inhalace akutní respirační selhání: tachypnoe, cyanosa, hypoxie Bilat infiltráty na RTG- nekardiální edém PaO2/FiO2 ratio < 200mmHg The medical history: acute onset of respiratory failure in combination with an underlying condition which has the potential to initiate a pulmonary inflammation. A recent frontal chest radiograph showing bilateral infiltrates. A clinical examination (and medical history), echocardiography or pulmonary artery catheterisation (PCWP <18 mmHg) excluding significant left ventricular heart failure. An arterial blood sample together with measurement of FiO2, showing a PaO2/FiO2 ratio <27 kPa for the diagnosis of ARDS and between 27 and 40 kPa for the diagnosis of ALI.
sepse), tkáňová ischemie, nekrozy, trauma tkání. pulmonární: pneumonie, aspirace, kontuze, inhalace. akutní respirační selhání: tachypnoe, cyanosa, hypoxie. Bilat infiltráty na RTG- nekardiální edém. PaO2/FiO2 ratio < 200mmHg. The medical history: acute onset of respiratory failure in combination with an underlying condition which has the potential to initiate a pulmonary inflammation. A recent frontal chest radiograph showing bilateral infiltrates. A clinical examination (and medical history), echocardiography or pulmonary artery catheterisation (PCWP <18 mmHg) excluding significant left ventricular heart failure. An arterial blood sample together with measurement of FiO2, showing a PaO2/FiO2 ratio <27 kPa for the diagnosis of ARDS and between 27 and 40 kPa for the diagnosis of ALI.")
3
Kdy indikovat UPV ARDS DF 30-35/min hypoxemie (na masce s O2)
nárůst paCO2 únava pacienta If the patient is fully awake, haemodynamically stable and is not fatigued there is no immediate need of ventilator support even if blood gases may indicate slight hypoxaemia. However, because almost all patients with ARDS require some form of ventilatory support, ventilator therapy should always be considered early in the disease process. If the patient is exhausted, has a respiratory rate above 30-35/min, blood gases indicate hypoxaemia (PaO2 <7-8 kPa) on oxygen via mask, an increasing carbon dioxide pressure in the arterial blood (PaCO2) or pH is below 7.3 (showing that the patient cannot maintain a normal pH by spontaneous breathing) ventilator therapy should be initiated expediently. If the patient is haemodynamically unstable but can maintain PaO2 above 8 kPa on oxygen via mask, haemodynamic support is indicated under careful ventilatory monitoring before invasive ventilatory support (intubation) is initiated.
 on oxygen via mask, an increasing carbon dioxide pressure in the arterial blood (PaCO2) or pH is below 7.3 (showing that the patient cannot maintain a normal pH by spontaneous breathing) ventilator therapy should be initiated expediently. If the patient is haemodynamically unstable but can maintain PaO2 above 8 kPa on oxygen via mask, haemodynamic support is indicated under careful ventilatory monitoring before invasive ventilatory support (intubation) is initiated.")
4
Cíle ventilační terapie
PaO2 >8 kPa SaO2 >90% nezpůsobit další postižení plic The goal for ventilatory therapy in ARF is to provide an adequate gas exchange (usually PaO2 >8 kPa, oxygen saturation of haemoglobin in arterial blood and pH ) without causing additional iatrogenic damage to lungs and other organs, i.e. a lung protective ventilatory strategy. In this context it is important to recognise that a ventilator can only replace the work done by respiratory muscles and not the gas exchange function of the lungs. However, by using lung recruitment manoeuvres, positive end-expiratory pressure and changing the inspired oxygen concentration, gas exchange may be improved and supported.
 without causing additional iatrogenic damage to lungs and other organs, i.e. a lung protective ventilatory strategy. In this context it is important to recognise that a ventilator can only replace the work done by respiratory muscles and not the gas exchange function of the lungs. However, by using lung recruitment manoeuvres, positive end-expiratory pressure and changing the inspired oxygen concentration, gas exchange may be improved and supported.")
5
Non invasive ventilation
při vědomí kooperace toleruje periody bez UPV pokud není příznívá odpověď do hodiny INTUBACE Shall we start a trial with non-invasive ventilation? Non-invasive ventilation (NIV) with continuous positive airway pressure (CPAP) may be considered in otherwise stable patients with hypoxaemia and without CO2 retention. Non-invasive positive pressure ventilation (NIPPV) is otherwise the preferred method in patients with ARF. NIPPV can only be considered if the staff members are experienced with the method and if the patient is: Fully conscious Cooperative Haemodynamically stable Tolerant of short periods without ventilatory support Able to take adequately large breaths Not fatigued
 with continuous positive airway pressure (CPAP) may be considered in otherwise stable patients with hypoxaemia and without CO2 retention. Non-invasive positive pressure ventilation (NIPPV) is otherwise the preferred method in patients with ARF. NIPPV can only be considered if the staff members are experienced with the method and if the patient is: Fully conscious. Cooperative. Haemodynamically stable. Tolerant of short periods without ventilatory support. Able to take adequately large breaths. Not fatigued.")
6
Intubace- selhání NIV Neadekvátní výměna plynů na NIV
těžká hypoxemie paO2 6-7 kPa acidosa 7,2, paCO2 >9 porucha vědomí nebo neprůchodnost dýchacích cest postižení CNS Intubation /tracheostomy The indications for intubation in ARF are: Inadequate gas exchange with non-invasive means (oxygen via mask or NIV) or When NIV is contraindicated or believed to be insufficient, e.g. Severe hypoxaemia (PaO2 <6-7 kPa) Severe respiratory acidosis (pH <7.2, PCO2 > 9-10 kPa) Semi-or unconsciousness or unable to keep upper airways free Concomitant central nervous system compromise (head injury, brain oedema due to meningitis or intracerebral bleeding, spinal injury) Acute surgery
 or. When NIV is contraindicated or believed to be insufficient, e.g. Severe hypoxaemia (PaO2 <6-7 kPa) Severe respiratory acidosis (pH <7.2, PCO2 > 9-10 kPa) Semi-or unconsciousness or unable to keep upper airways free. Concomitant central nervous system compromise (head injury, brain oedema due to meningitis or intracerebral bleeding, spinal injury) Acute surgery.")
7
Intubace personální a technické vybavení rychlý úvod
laryngoskopy, odsávání, zavaděče náhradní postupy: laryngeální maska, fibroptická intubace, coniotomie rychlý úvod selickův hmat- tlak na krikoidní chrupavku anestetikum, (SCHIJ) ověření polohy tracheální rourky auskultace kapnografie RTG
 ověření polohy tracheální rourky. auskultace. kapnografie. RTG.")
8
Tracheostomie po 7-14 dnech UPV v případě předpokládané delší UPV
operační nebo punkční usnadní odpojení od ventilátoru

9
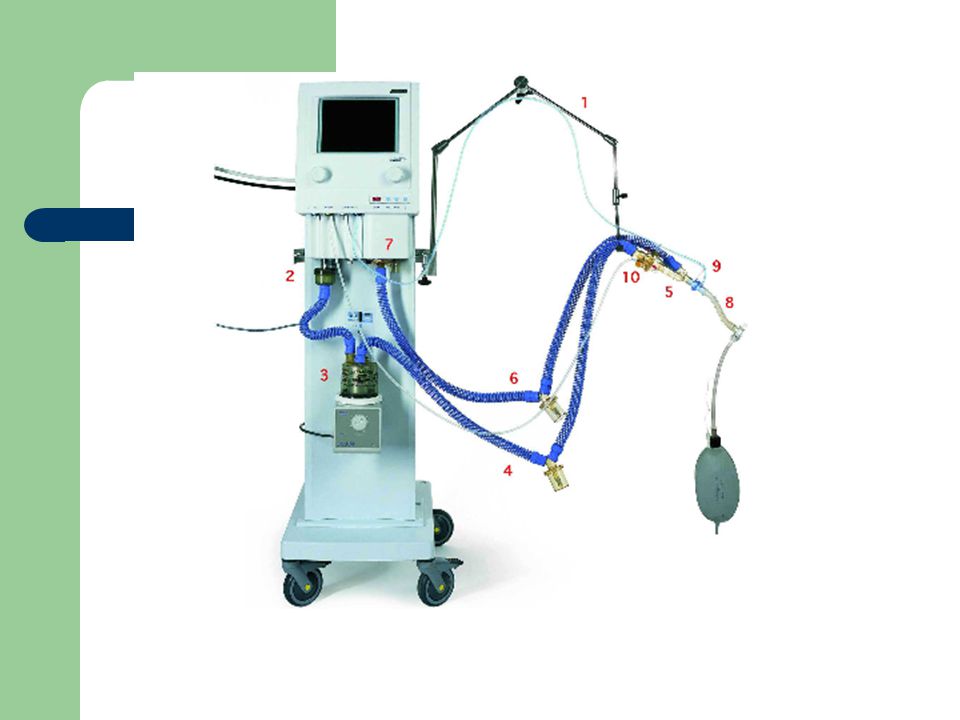
UPV- prostředky servoventilátor zvlhčovač
přivod O2, vzduchu centrální přívod , vysoký tlak směšovač plynů chopně- inspirační , expirační, computer, zpětné vazby monitor bezpečnostní systémy: hlašení nepřítomnosti ventilace, nízkého O2, vysokých tlaků dýchací okruhy trigger- umožňuje spouštět dech podle pacientova úsilí. zvlhčovač nutná 100% vlhkost inspirované směsi při orotracheáolní intubaci

12
Způsoby UPV UPV= pozitivní přetlak základní proměnná – tlak nebo objem
tlak cm H2O, nad 30 cm H2O nebezpečné, možnost ventilator induced lung injury objem 6-8 ml/kg ideální hmotnosti 480 ml

13
PEEP prevence kolapsu otevřených alveolů
overdistension otevřených plicních regionů nastavení: podle oxygenace, podle nejlepší poddajnosti plic, empiricky Whether positive end-expiratory pressure (PEEP) is important in preventing lung injury or is associated with improved outcome in patients with ARF is not yet known Applying PEEP is not a recruitment manoeuvre PEEP May prevent collapse of open and perfused lung regions and thus maintain arterial oxygenation. In itself does not recruit collapsed lung regions, since recruitment is an inspiratory phenomenon and PEEP is an expiratory one. May indirectly cause a high end-inspiratory pressure which may open up collapsed lung regions and thus decrease the intrapulmonary shunt fraction and improve arterial oxygenation. If inadequately set, may induce overdistension of already open lung regions.
 is important in preventing lung injury or is associated with improved outcome in patients with ARF is not yet known. Applying PEEP is not a recruitment manoeuvre. PEEP. May prevent collapse of open and perfused lung regions and thus maintain arterial oxygenation. In itself does not recruit collapsed lung regions, since recruitment is an inspiratory phenomenon and PEEP is an expiratory one. May indirectly cause a high end-inspiratory pressure which may open up collapsed lung regions and thus decrease the intrapulmonary shunt fraction and improve arterial oxygenation. If inadequately set, may induce overdistension of already open lung regions.")
14
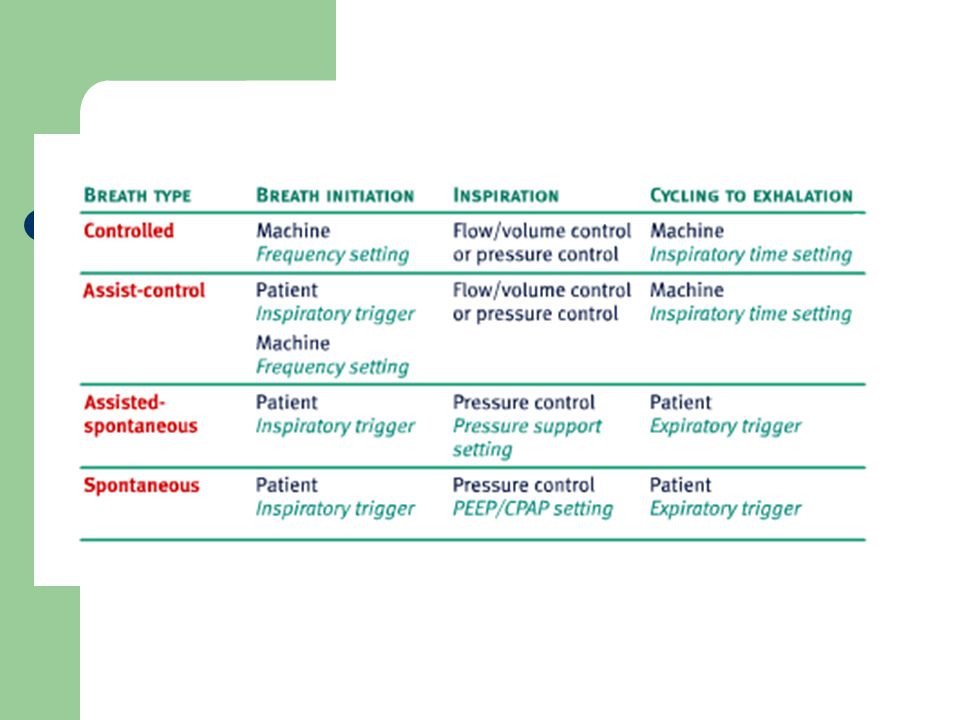
UPV režimy VCV- Volume-Controlled Ventilation
PCV- Pressure-Controlled Ventilation SIMV - Synchronised Intermittent Mandatory Ventilation PSV- Pressure Support Ventilation (PSV)
")
16
Parametry UPV TV tidal volume= dechový objem
PIP = peak inspiratory pressure PEEP = positive endexpiratory pressure DF= dechová frekvence I:E- poměr trvání inspiria: expiria (1:2)
")
17
kontrola UPV Klinicky nejsou známky respir. insuff.
není interference= nesoulad s ventilační cyklem, např. inspirium pacienta během expiria ventilátori „thorakoabdominální nesoulad“ kontrola krevních plynů, ASTRUP paO2, paCO2

18
Laboratorní sledování UPV
paO2- závislé na Oběhu FiO2 PEEP V´CO2- produkce CO2, V´A alveolární ventilace

19
Infekce a UPV riziko VAP- ventilator associated pneumonia
nedostatečné reflexy k odstraňování hlenu kolonizace dýchacího traktu bakteriemi nedostatečná těsnost manžety TR- mikroaspisrace

20
Prone position homohennější distribuce ventilace
zlepšení oxygenace u ARDS Standardní poloha: supine, elevace horní části těla o 30st Prone position Although prone position has not been demonstrated to increase survival rate, it might be considered in severe ARDS to improve oxygenation. Using the prone position requires an increased number of staff. In the prone position compared with the supine position, pleural pressure is more homogenously distributed causing increased ventilation to the dorsal regions. Likewise, the perfusion is more homogenous. This results in an improved ventilation-perfusion ratio. Oxygenation increases in 70% (60-95%) of patients in the prone position. This increase is usually seen within minutes or within the first 1-2 hours in about 60-70% of patients. Usually, the positive effects are maintained when the patient is turned back to the supine position. The response is more favourable in patients with extra-pulmonary than in pulmonary ARDS.
 of patients in the prone position. This increase is usually seen within minutes or within the first 1-2 hours in about 60-70% of patients. Usually, the positive effects are maintained when the patient is turned back to the supine position. The response is more favourable in patients with extra-pulmonary than in pulmonary ARDS.")
21
fyziotherapie hygiena DU odsávání ze subglotického prostoru
odávání z TR poklepové masáže hrudníku vibrační masáže atd. Physiotherapy Oxygenation might be improved by turning the patient lateral with best lung dependent or letting the patient sit up Lung physiotherapy has not conclusively been shown to improve outcome. However, careful hygiene of the mouth and subglottic regions by e.g. suctioning may reduce the incidence of nosocomial infections. Endotracheal suctioning should only be done on demand because suctioning in these patients can induce severe lung collapse and hypoxaemia. In addition, physiotherapy and endotracheal suctioning increase the metabolic

22
zvlhčovač nutná 100% vlhkost inspirované směsi na úrovni kariny
Zvlhčovače teplné-heated humidifiers HME: heat and moisture exchangers

23
Komplikace UPV- hemodynamika
snížení venosního návratu při zvýšeném nitrohrudním tlaku během UPV snížení kardiálního výdeje Haemodynamics If hypotension occurs during a lung recruitment manoeuvre, suspect hypovolaemia or tension pneumothorax. Patients with septic shock are also susceptible Because ventilator therapy generates positive pressure in the thorax it will hamper the venous return and also the right ventricular ejection by compressing pulmonary capillaries, and thus decrease cardiac output. The mean airway pressure is probably more important than PEEP or the peak airway pressure. The intermittent decrease in venous filling caused by the positive intrathoracic pressure produces a variation in systemic arterial pressure (systolic pressure or pulse pressure variation). If signs of decreased peripheral perfusion occur, e.g. hypotension, decreased urine output, metabolic acidosis or lactacidosis, i.v. fluids should be given until the pressure variations are minimised, or the intracardiac filling is adequate as judged by echocardiography or by intrathoracic intravascular volume measurements. The filling pressures (central venous and pulmonary artery occlusion pressure) may be elevated and may not reliably indicate the volume status of the heart. Administration of i.v. fluids is usually enough to counteract the influence on the cardiac filling by the positive airway pressure. pokles orgánové perfůze tekutiny i.v.- působí proti neg. hemodyn. účinkům UPV
. If signs of decreased peripheral perfusion occur, e.g. hypotension, decreased urine output, metabolic acidosis or lactacidosis, i.v. fluids should be given until the pressure variations are minimised, or the intracardiac filling is adequate as judged by echocardiography or by intrathoracic intravascular volume measurements. The filling pressures (central venous and pulmonary artery occlusion pressure) may be elevated and may not reliably indicate the volume status of the heart. Administration of i.v. fluids is usually enough to counteract the influence on the cardiac filling by the positive airway pressure. pokles orgánové perfůze. tekutiny i.v.- působí proti neg. hemodyn. účinkům UPV.")
24
Komplikace UPV- ventilator-induced lung injuries (VILI)
mikroskopické (biotrauma) vysoké tlaky (barotrauma ) vysoke objemy (volutrauma) emphyzém intersticiální pneumothorax subkutánní mediastinální (retroperitoneální) (peritoneální)
 vysoké tlaky (barotrauma ) vysoke objemy (volutrauma) emphyzém. intersticiální. pneumothorax. subkutánní. mediastinální. (retroperitoneální) (peritoneální)")
25
minimálně invazivní ventilace
Fyziologie: dýchání negativním pod tlakem Umělá plicní ventilace: dýchání pozitivním přetlakem Tlak v DC: spont + UPV - Rizika UPV: (ventilator associated lung injury - VALI) barotrauma (vysoké tlaky v DC) ….P plat < 35 cm H2O volumotrauma - vysoké střižní síly (shear forces) - cyklické otevírání a zavírání části plic (atelektáza) biotrauma - indukce inflamace v plicích...šíření do organizmu Zásady:dostatečný PEEP (optimálně dle plicní mechaniky) malé dechové objemy max 10 ml/kg IBW frekvence jen nutná - permisivní hyperkapnie
 barotrauma (vysoké tlaky v DC) ….P plat < 35 cm H2O. volumotrauma - vysoké. střižní síly (shear forces) - cyklické otevírání a zavírání. části plic (atelektáza) biotrauma - indukce inflamace v plicích...šíření do organizmu. Zásady:dostatečný PEEP (optimálně dle plicní mechaniky) malé dechové objemy max 10 ml/kg IBW. frekvence jen nutná - permisivní hyperkapnie.")
27
Weaning- odpojení od ventilátoru
Odpojení a extubace Kritéria weaningu Při vědomí, kooperativní Stabilní oběh Bez sepse Dostatečná spont. ventilace- svalová síla Dostatečný TV při PSV Schopen odkašlat

Podobné prezentace




















 –pravá - 3 laloky, levá - 2 laloky –plicní váčky složeny z plicních sklípků (alveol) opletené kapilárami,>")
