Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
(Maligní) Lymfomy
 Lymfomy")
2
Maligní lymfoproliferace
Def: klonální onem. lymfocytů v různém stádiu ontogeneze WHO 1999: Prekursor Periferní HL ALL (B,T) LBL NHL HL: Hodgkinův lymfom, NHL: nonhodgkinské lymfomy, ALL: akutní lymfoblastová leukémie, LBL: lymfoblastický lymfom
 LBL. NHL. HL: Hodgkinův lymfom, NHL: nonhodgkinské lymfomy, ALL: akutní lymfoblastová leukémie, LBL: lymfoblastický lymfom.")
3
Thomas Hodgkin 1832 „On Some Morbid Appearances of the Exorband Glands
and Spleen“ . Onemocnění poprvé popsal u sedmi pacientů v roce 1832 anglický patolog Thomas Hodgkin. Předpokládal, že masivní zvětšení krčních, nitrohrudních a abdominálních lymfatických uzlin a sleziny není reaktivní nebo zánětlivé etiologie, ale, že se spíše jedná o nádorovou proliferaci.

4
Hodgkinův lymfom - HL Incidence v závislosti na věku bimodální: nejvíce mezi rokem a rokem věku Patologie: přítomnost buněk Reedové-Stenberga (RS buňky), resp. Hodgkinových buněk Etiologie: nejasná, role EBV ne zcela objasněná, v 80% RS buněk je přítomen genom EBV. EBV hraje pravděpodobně částěčnou roli v patogenezi HL.
, resp. Hodgkinových buněk. Etiologie: nejasná, role EBV ne zcela objasněná, v 80% RS buněk je přítomen genom EBV. EBV hraje pravděpodobně částěčnou roli v patogenezi HL.")
5
HL - histologické subtypy - WHO klasifikace
Nodulární skleróza: nejčastější forma HL (50-80%) 2. Smíšená celularita: druhá nejčastější forma HL (20-30%) 3. Klasický HL bohatý na lymfocyty 4. Lymfocytová deplece 5. Lymfocytová predominance (paragranulom)
 2. Smíšená celularita: druhá nejčastější forma HL (20-30%) 3. Klasický HL bohatý na lymfocyty. 4. Lymfocytová deplece. 5. Lymfocytová predominance (paragranulom)")
6
Hodgkinův lymfom (HL), klinické příznaky
lymfadenopatie + konstituční příznaky: subfebrilie nebo horečky nejasné etio, hubnutí, noční poty, dyspnoe, bolest na hrudi, někdy slabost, pruritus (svědění), alkoholová bolest aj.
, alkoholová bolest aj.")
7
Hodgkinův lymfom (HL), klinické příznaky
lymfadenopatie + - konstituční příznaky: subfebrilie nebo horečky nejasné etio, hubnutí, noční poty, dyspnoe, bolest na hrudi, někdy slabost, pruritus (svědění), alkoholová bolest aj. - vzácně: paraneoplastické syndromy (AIHA, ITP), demyelinizační syndrom, další neurologické syndromy, nefrotický syndrom.
, alkoholová bolest aj. - vzácně: paraneoplastické syndromy (AIHA, ITP), demyelinizační syndrom, další neurologické syndromy, nefrotický syndrom.")
8
Hodgkinův lymfom (HL), klinické příznaky
lymfadenopatie + - konstituční příznaky: subfebrilie nebo horečky nejasné etio, hubnutí, noční poty, dyspnoe, bolest na hrudi, někdy slabost, pruritus (svědění), alkoholová bolest aj. - vzácně: paraneoplastické syndromy (AIHA, ITP), demyelinizační syndrom, další neurologické syndromy, nefrotický syndrom. - výjimečně: CNS symptomy způsobené přímo HL
, alkoholová bolest aj. - vzácně: paraneoplastické syndromy (AIHA, ITP), demyelinizační syndrom, další neurologické syndromy, nefrotický syndrom. - výjimečně: CNS symptomy způsobené přímo HL.")
9
Posouzení lymfadenopatie fyzikálním vyšetřením
Jednotlivá uzlina, region Umístění Rozšířené postižení Generalizovaná lymfadenopatie Symetrie Velikost Citlivost Konzistence Postižení okolí Lymphadenopattie vs. Pseudolymphadenopatie (např. sialoadenitis)
")
10
Lympfatické orgány Waldeyerův okruh Lymfatické uzliny Thymus Slezina
Kostní dřeň

11
Lymfadenopatie

12
Příčiny lyfadenopatie
Infekce EBV (IM), CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc.
, CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I. Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc.")
13
Příčiny lyfadenopatie
Infekce EBV (IM), CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc. Autoimunitní choroby RA, SLE, dermatomyositis, MCTD, Sjögrenův sy
, CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I. Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc. Autoimunitní choroby. RA, SLE, dermatomyositis, MCTD, Sjögrenův sy.")
14
Příčiny lyfadenopatie
Infekce EBV (IM), CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc. Autoimunitní choroby RA, SLE, dermatomyositis, MCTD, Sjögrenův sy Maligní příčiny Hematologické: Hodgkinův lymfom, NHL, CLL, Waldenströmova makroglobulinemie, některé akutní leukémie (ALL), systémová mastocytosa. Metastické karcinomy: prsu, plic, ledvin, žaludku, melanom …
, CMV, IH, postvakcinační lymfadenitis, adenovirus, VZV, HIV, HTLV-I. Staphylococcus, Streptococcus spec.,TB, atypická mykobakteria, syphilis, nemoc kočičího škrábnutí, Chlamydie (lymf. venereum) Toxoplasmosa, histoplasmosis, coccidiomycosa, tyfus, filariosa, etc. Autoimunitní choroby. RA, SLE, dermatomyositis, MCTD, Sjögrenův sy. Maligní příčiny. Hematologické: Hodgkinův lymfom, NHL, CLL, Waldenströmova makroglobulinemie, některé akutní leukémie (ALL), systémová mastocytosa. Metastické karcinomy: prsu, plic, ledvin, žaludku, melanom …")
15
Časté příčiny lymfadenopatie podle lokalizace
Ingvinální nebo axilární adenopatie 1cm: obvykle benigní Cervikální adenopatie: infekce, karcinomy (konzistence), lymfomy. Sialoadenitida (pseudolymfadenopatie) Mediastinální : lymfomy (přední mediastinum), sarkoidosa, metastazující ca Izolovaná axilární : infekce, Ca prsu, lymfom Izolovaná ingvinální (signifikantní): infekce (též venerické), lymphomy, metastazující Ca Generalizovaná lymfadenopatie: infekce (EBV, HIV, etc.), maligní lymfomy, CLL
, lymfomy. Sialoadenitida (pseudolymfadenopatie) Mediastinální : lymfomy (přední mediastinum), sarkoidosa, metastazující ca. Izolovaná axilární : infekce, Ca prsu, lymfom. Izolovaná ingvinální (signifikantní): infekce (též venerické), lymphomy, metastazující Ca. Generalizovaná lymfadenopatie: infekce (EBV, HIV, etc.), maligní lymfomy, CLL.")
16
HL – stanovení diagnózy
anamnéza fyzikální vyšetření : lymfadenopatie (gumovitá konzistence) + - pleurální efuze +- splenomegalie Laboratorní: ESR elevace, může být anemie, lymfopenie, eosinofilie. Biochemie: může být elevace: LDH, beta2 mikroglobulin, CRP RTG S+P: masa(bulk) v předním mediastinu, mohou být pleurální či perikardiální efuze CT, PET, USG Vyšetření kostní dřeně
 + - pleurální efuze. +- splenomegalie. Laboratorní: ESR elevace, může být anemie, lymfopenie, eosinofilie. Biochemie: může být elevace: LDH, beta2 mikroglobulin, CRP. RTG S+P: masa(bulk) v předním mediastinu, mohou být pleurální či perikardiální efuze. CT, PET, USG. Vyšetření kostní dřeně.")
17
HL – stanovení diagnózy
anamnéza fyzikální vyšetření : lymfadenopatie (gumovitá konzistence) + - pleurální efuze +- splenomegalie Laboratorní: ESR elevace, může být anemie, lymfopenie, eosinofilie. Biochemie: může být elevace: LDH, beta2 mikroglobulin, CRP RTG S+P: masa(bulk) v předním mediastinu, mohou být pleurální či perikardiální efuze CT, PET, USG Vyšetření kostní dřeně HISTOLOGIE (LU) STAGING
 + - pleurální efuze. +- splenomegalie. Laboratorní: ESR elevace, může být anemie, lymfopenie, eosinofilie. Biochemie: může být elevace: LDH, beta2 mikroglobulin, CRP. RTG S+P: masa(bulk) v předním mediastinu, mohou být pleurální či perikardiální efuze. CT, PET, USG. Vyšetření kostní dřeně. HISTOLOGIE (LU) STAGING.")
18
Stanovení klinického stadia HL / NHL
- Ann Arbor klasifikace Stadium I – 1 skupina uzlin nebo 1 extralymf. orgán Stadium II – 2 nebo více skupin LU na téže straně bránice Stadium III – postižení nad i pod bránicí + /- 1 extralymf. Orgán (Slezina – S, Extralymfatický oprgán E) Stadium IV – disseminoivané nebo difúzní postižení extralymfatického orgánu postižení
 Stadium IV – disseminoivané nebo difúzní postižení extralymfatického orgánu postižení.")
19
Stanovení klinického stadia HL / NHL
- Ann Arbor klasifikace Stadium I – 1 skupina uzlin nebo 1 extralymf. orgán Stadium II – 2 nebo více skupin LU na téže straně bránice Stadium III – postižení nad i pod bránicí + /- 1 extralymf. Orgán (Slezina – S, Extralymfatický oprgán E) Stadium IV – disseminoivané nebo difúzní postižení extralymfatického orgánu postižení B symptomy: noční poty, febrilie nejasné etio, váhový úbytek nad 10%
 Stadium IV – disseminoivané nebo difúzní postižení extralymfatického orgánu postižení. B symptomy: noční poty, febrilie nejasné etio, váhový úbytek nad 10%")
20
Léčba HL a) Časná stádia: chemoterapie (ABVD) + radioterapie postižené oblasti = involved field (IF) b) Intermediární stádia : chemoterapie ABVD nebo BEACOPP + radioterapie IF c) Pokročilá stádia: chemoterapie BEACOPP („eskalovaný BEACOPP“) ABVD: Adriamycin, Blemocyin, Vinblastin, Dakarbazin BEACOPP: Bleomycin, Etoposid, Adriamycin, Cyklofosfamid, Vincristin, Prokarbazin, Prednison Prognoza: % vyléčeni Komplikace: sekundární malignity
 Intermediární stádia : chemoterapie ABVD nebo BEACOPP + radioterapie IF. c) Pokročilá stádia: chemoterapie BEACOPP („eskalovaný BEACOPP ) ABVD: Adriamycin, Blemocyin, Vinblastin, Dakarbazin. BEACOPP: Bleomycin, Etoposid, Adriamycin, Cyklofosfamid, Vincristin, Prokarbazin, Prednison. Prognoza: % vyléčeni. Komplikace: sekundární malignity.")
21
incidence narůstá s věkem
NHL vs. HL incidence narůstá s věkem 30%primárně extranodální CNS postižení časté Histologická a biologická variabilita prognóza různá Stabilní incidence – bimodální 99% primárně nodální postižení CNSpostižení velmi vzácně 5 histol. subtypů % vyléčitelnost

22
Co je to NHL? Back to TOC Neoplastická transformace normální lymfoidní buňky v lymfatické tkáni Kostní dřeň – KD (bone marrow BM) LU Slezina Thymus >30 histologických variant pocházejících ze 3 typů buněk: - B buňky T buňky Natural killer (NK) bb Key Point NHL is a neoplastic transformation of normal lymphoid cells residing primarily in lymphoid tissue. It is important to recognize that NHL is not a single disease entity, but encompasses more than 30 different histologies. Background The lymphoid tissues include BM, the lymph nodes, the spleen, and the thymus. The different histologies of NHL arise from 3 cell types: B cells, T cells, and NK cells. References 1. DeVita et al, eds. Cancer Principles & Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008. 2. Non-Hodgkin’s Lymphoma Cyberfamily Web site. Accessed November 15, 2009. DeVita et al, eds. Cancer Principles & Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008; Non-Hodgkin’s Lymphoma Cyberfamily Web site. Accessed November 15, 2009.
 bb. Key Point. NHL is a neoplastic transformation of normal lymphoid cells residing primarily in lymphoid tissue. It is important to recognize that NHL is not a single disease entity, but encompasses more than 30 different histologies. Background. The lymphoid tissues include BM, the lymph nodes, the spleen, and the thymus. The different histologies of NHL arise from 3 cell types: B cells, T cells, and NK cells. References. 1. DeVita et al, eds. Cancer Principles & Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; Non-Hodgkin’s Lymphoma Cyberfamily Web site. Accessed November 15, DeVita et al, eds. Cancer Principles & Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008; Non-Hodgkin’s Lymphoma Cyberfamily Web site. Accessed November 15,")
23
NH lymfomy – věk incidence v letech 1973 - 1975
ve srovnání s roky

24
Key Point The incidence of NHL in the US has been increasing over the last 3 decades ( ). (See graph on slide.) Background Trends in age-adjusted Surveillance Epidemiology and End Results (SEER) incidence rates, including both sexes, all races, and all ages, indicate a 3.6% increase in incidence of NHL from , a 0.6% increase in incidence from , and a 2.1% decrease in incidence from (Data not shown on slide.) References 1. Jemal et al. Cancer J Clin. 2009;59: 2. Horner et al, eds. SEER Cancer Statistics Review, Bethesda, MD: National Cancer Institute. Accessed November 4, 2009.
 incidence rates, including both sexes, all races, and all ages, indicate a 3.6% increase in incidence of NHL from , a 0.6% increase in incidence from , and a 2.1% decrease in incidence from (Data not shown on slide.) References. 1. Jemal et al. Cancer J Clin. 2009;59: Horner et al, eds. SEER Cancer Statistics Review, Bethesda, MD: National Cancer Institute. Accessed November 4,")
25
NHL – incidence a mortalita (1982 – 2001)
")
26
Key Point The global incidence of NHL varies by region, with the highest incidence rates observed in Northern America and the lowest in China. Background Northern America, Australia/New Zealand, and Western, Northern, and Southern Europe have the highest incidence rates, whereas Northern, Middle, and Southern Africa, Eastern Europe, South Central Asia, and China have the lowest incidence rates. The incidence of NHL is higher in men than in women in all regions except in Middle Africa. Reference Parkin et al. CA Cancer J Clin. 2005; 55:

27
NHL: etiologie Víceméně neznámá
Germinální mutace (AT, Wiskot Aldrich, NBS) Infekce (EBV (+ malárie), H.I.V., HSV-8, HCV, H.pylori, Bor. burgdorferi) Chemikálie (org. rozpouštědla, barvy na vlasy, chemoterapie) Imunosuprese (transplantace orgánů) Autoimunitní choroby (SLE, Sjög.sy.)
 Infekce (EBV (+ malárie), H.I.V., HSV-8, HCV, H.pylori, Bor. burgdorferi) Chemikálie (org. rozpouštědla, barvy na vlasy, chemoterapie) Imunosuprese (transplantace orgánů) Autoimunitní choroby (SLE, Sjög.sy.)")
28
Pokročilá stádia: III, IV
NHL: staging Ann Arbor system jako u HL Časná stádia: I, II Pokročilá stádia: III, IV

29
NHL Incidence v USA (2009) Back to TOC V USA cca 65,980 lidem bude diagnostikován NHL1 Predominance u letých2 Nejčastější neoplasma Asi 452,723 lidí aktuálně žije s NHL, odhadem 19,500 na tuto dg zemře1 9. nejčastější nádorová příčina úmrtí u mužů 6. u žen Key Point In the US in 2009, approximately 65,980 people will be diagnosed with NHL, about 452,723 people are currently living with the disease, and an estimated 19,500 people will die of NHL. Background NHL is the 9th most common cause of cancer death in men and 6th most common cause of cancer death in women. Most patients with NHL are between years of age. References 1. Leukemia and Lymphoma Society Web site. page.adp?item_id=8965#_moreinfo. Accessed October 16, 2009. 2. American Cancer Society Web site. Cancer_Statistics_2009_Presentation.asp. Accessed October 16, 2009. 3. Data on file, Celgene. 1. Leukemia and Lymphoma Society Web site #_moreinfo. Accessed October 16, 2009; 2. Data on file, Celgene.

30
Globální NHL Incidence (2007)
Back to TOC Odhadem 196,298 případů NHL diagnostikováno celosvětově u mužů v 20071* Přibližně 111,126 úmrtí (u mužů)1* Globálně – narůstající incidence NHL 2 150% nárůst za 30 let Nárůst o 4% ročně od 1970 Úmrtnost narůstající o 2% ročně ( vyšší nárůst pouze u ca plic žen a maligního melanomu) Key Point The global incidence of NHL in men in 2007 was estimated at 196,298 cases, and about 111,126 deaths occurred in men worldwide. (Note: the global incidence rates in women were not reported.) Background The worldwide incidence of NHL has been increasing by about 4% annually since the 1970s and the mortality rate is rising by about 2% each year. References 1. American Cancer Society Web site. and_Figures_2007_rev2.pdf. Accessed October 16, 2009. 2. American Cancer Society Web site. Cancer_Statistics_2009_Presentation.asp. Accessed October 16, 2009. *Incidence rates were only reported for top 10 cancer sites in each sex; no data for specific incidence rates in women available. 1. American Cancer Society Web site. _2007_rev2.pdf. Accessed October 16, 2009; 2. American Cancer Society Web site. docroot/PRO/content/PRO_1_1_Cancer_Statistics_2009_Presentation.asp. Accessed October 16, 2009.
1* Globálně – narůstající incidence NHL % nárůst za 30 let. Nárůst o 4% ročně od Úmrtnost narůstající o 2% ročně ( vyšší nárůst pouze u ca plic žen a maligního melanomu) Key Point. The global incidence of NHL in men in 2007 was estimated at 196,298 cases, and about 111,126 deaths occurred in men worldwide. (Note: the global incidence rates in women were not reported.) Background. The worldwide incidence of NHL has been increasing by about 4% annually since the 1970s and the mortality rate is rising by about 2% each year. References. 1. American Cancer Society Web site. and_Figures_2007_rev2.pdf. Accessed October 16, American Cancer Society Web site. Cancer_Statistics_2009_Presentation.asp. Accessed October 16, *Incidence rates were only reported for top 10 cancer sites in each sex; no data for specific incidence rates in women available. 1. American Cancer Society Web site. _2007_rev2.pdf. Accessed October 16, 2009; 2. American Cancer Society Web site. docroot/PRO/content/PRO_1_1_Cancer_Statistics_2009_Presentation.asp. Accessed October 16,")
31
Key Point Different histologic subtypes of NHL occur at varying frequencies. Two of the most common histologic subtypes of NHL in adults include DLBCL (31% of all NHL) and FL (22% of all NHL). MCL occurs at a frequency of 6%. Reference Armitage et al. J Clin Oncol. 1998;16:
 and FL (22% of all NHL). MCL occurs at a frequency of 6%. Reference. Armitage et al. J Clin Oncol. 1998;16:")
32
Key Point The figure depicts a differentiation scheme, showing the postulated normal counterpart of many of the T- and B-cell neoplasms that can currently be recognized. Background The malignant cells of MCL correlate with mantle cells, the malignant cells of DLBCL correlate with B-immunoblasts and/or centroblasts, and the malignant cells of FL correlate with centrocytes. Immunohistochemical markers associated with each malignant cell type aid in the differentiation and diagnosis of the different B-cell lymphomas. Reference DeVita et al, eds. Cancer Principles & Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008.

33
Klasifikace lymfomů Revised European-American Lymphoma (REAL):
Back to TOC Revised European-American Lymphoma (REAL): (1990s) REAL klasifikace , založena na imunofenotypizaci a cytogenetice; rozlišuje jasné klinicko-patologické NHL entity World Health Organization (WHO): (2001) klasifikace, vycházející ze tří hlavních typů buněk (Sep 2008) revize: 30 subtypů lymfomů ze zralých B buněk 21 subtypů lymfomů z T- a NK- bb 9 prekurzorových B-cell lymfomů/leukémií 5 typů Hodgkinova lymfomu Key Point There have been several classification schemes for lymphoma which have been revised based on increased knowledge and understanding of the nature of NHL. Background The REAL classification is based on immuno-phenotypic and genetic features. The 2001 WHO classification is based on the 3 major cell types (B cell, T cell, and NK cell). The 2008 WHO classification updated the various lymphoma subtypes. References 1. Isaacson. Clin Oncol (R Coll Radiol). 1995;7: 2. Jaffe et al. Blood. 2008;112: 3. Vardiman et al. Blood. 2009;114: Jaffe et al. Blood. 2008;112: ; Vardiman et al. Blood. 2009;114:
: (1990s) REAL klasifikace , založena na imunofenotypizaci a cytogenetice; rozlišuje jasné klinicko-patologické NHL entity. World Health Organization (WHO): (2001) klasifikace, vycházející ze tří hlavních typů buněk. (Sep 2008) revize: 30 subtypů lymfomů ze zralých B buněk. 21 subtypů lymfomů z T- a NK- bb. 9 prekurzorových B-cell lymfomů/leukémií. 5 typů Hodgkinova lymfomu. Key Point. There have been several classification schemes for lymphoma which have been revised based on increased knowledge and understanding of the nature of NHL. Background. The REAL classification is based on immuno-phenotypic and genetic features. The 2001 WHO classification is based on the 3 major cell types (B cell, T cell, and NK cell). The 2008 WHO classification updated the various lymphoma subtypes. References. 1. Isaacson. Clin Oncol (R Coll Radiol). 1995;7: Jaffe et al. Blood. 2008;112: Vardiman et al. Blood. 2009;114: Jaffe et al. Blood. 2008;112: ; Vardiman et al. Blood. 2009;114:")
34
Revidovaná WHO klasifikace : 2008
Back to TOC B-cell neoplasms Precursor B-cell neoplasm: precursor B-acute lymphoblastic leukemia/lymphoblastic lymphoma (LBL). Peripheral (“Mature”) B-cell neoplasms. B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma. B-cell prolymphocytic leukemia. Lymphoplasmacytic lymphoma/immunocytoma. MCL. – mantle cell lymfom – lymfom z plášťových buněk FL. – folikulární lymfom Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphatic tissue (MALT) type. Nodal marginal zone B-cell lymphoma ( monocytoid B-cells). Splenic marginal zone lymphoma ( villous lymphocytes). Hairy cell leukemia. Plasmacytoma/plasma cell myeloma. DLBCL. - Difuzní velkobuněčný lymfom Burkitt lymphoma. Key Point The WHO classification system was updated in 2008 and provides an internationally agreed upon, clinically relevant classification system using histologic, phenotypic, clinical, and genetic data that can be used worldwide. Background The updated WHO classification system divides B-cell neoplasms into 2 major categories: precursor B-cell neoplasms and peripheral (“mature”) B-cell neoplasms. A discussion of each of these neoplasms is beyond the scope of this presentation, which will focus on 3 of the most common peripheral B-cell neoplasms: DLBCL, MCL, and FL. References 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; 2008. 2. Jaffe et al. Blood. 2008;112: 3. Vardiman et al. Blood. 2009;114: Jaffe et al. Blood. 2008;112: ; Vardiman et al. Blood. 2009;114:
. Peripheral ( Mature ) B-cell neoplasms. B-cell chronic lymphocytic leukemia/small lymphocytic lymphoma. B-cell prolymphocytic leukemia. Lymphoplasmacytic lymphoma/immunocytoma. MCL. – mantle cell lymfom – lymfom z plášťových buněk. FL. – folikulární lymfom. Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphatic tissue (MALT) type. Nodal marginal zone B-cell lymphoma ( monocytoid B-cells). Splenic marginal zone lymphoma ( villous lymphocytes). Hairy cell leukemia. Plasmacytoma/plasma cell myeloma. DLBCL. - Difuzní velkobuněčný lymfom. Burkitt lymphoma. Key Point. The WHO classification system was updated in 2008 and provides an internationally agreed upon, clinically relevant classification system using histologic, phenotypic, clinical, and genetic data that can be used worldwide. Background. The updated WHO classification system divides B-cell neoplasms into 2 major categories: precursor B-cell neoplasms and peripheral ( mature ) B-cell neoplasms. A discussion of each of these neoplasms is beyond the scope of this presentation, which will focus on 3 of the most common peripheral B-cell neoplasms: DLBCL, MCL, and FL. References. 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; Jaffe et al. Blood. 2008;112: Vardiman et al. Blood. 2009;114: Jaffe et al. Blood. 2008;112: ; Vardiman et al. Blood. 2009;114:")
35
Revidovaná WHO klasifikace : 2008
Back to TOC T-cell and putative NK-cell neoplasms Precursor T-cell neoplasm: precursor T-acute lymphoblastic leukemia/LBL. Peripheral T-cell and NK-cell neoplasms. T-cell chronic lymphocytic leukemia/prolymphocytic leukemia. T-cell granular lymphocytic leukemia. Mycosis fungoides/Sézary syndrome. Peripheral T-cell lymphoma, not otherwise characterized. Hepatosplenic gamma/delta T-cell lymphoma. Subcutaneous panniculitis-like T-cell lymphoma. Angioimmunoblastic T-cell lymphoma. Extranodal T-/NK-cell lymphoma, nasal type. Enteropathy-associated T-cell lymphoma. Adult T-cell lymphoma/leukemia (human T-lymphotrophic virus [HTLV] 1+). Anaplastic large cell lymphoma, ALK+. Anaplastic large cell lymphoma, ALK-. Aggressive NK-cell leukemia. Key Point The updated 2008 WHO classification system additionally provided a clinically relevant classification system for stratifying neoplasms derived from T-cell and putative NK-cell origins. Background T-cell and putative NK-cell neoplasms are further stratified into precursor vs peripheral (“mature”) neoplasms, and then subcategorized into more specific T- or NK-cell disease states. References 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; 2008. 2. Jaffe et al. Blood. 2008;112: Jaffe et al. Blood. 2008;112:
. Anaplastic large cell lymphoma, ALK+. Anaplastic large cell lymphoma, ALK-. Aggressive NK-cell leukemia. Key Point. The updated 2008 WHO classification system additionally provided a clinically relevant classification system for stratifying neoplasms derived from T-cell and putative NK-cell origins. Background. T-cell and putative NK-cell neoplasms are further stratified into precursor vs peripheral ( mature ) neoplasms, and then subcategorized into more specific T- or NK-cell disease states. References. 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; Jaffe et al. Blood. 2008;112: Jaffe et al. Blood. 2008;112:")
36
WHO klasifikace NHLdle průběhu onemocnění
Back to TOC Indolentní Agresivní FL (follicular small cleaved cell [Grade 1], follicular mixed small cleaved and large cell [Grade 2], diffuse small cleaved cell) CLL/SLL LL (Waldenström’s macroglobulinemia) Extranodal marginal zone B-cell lymphoma (MALT lymphoma) Nodal marginal zone B-cell lymphoma (monocytoid B-cell lymphoma) Splenic marginal zone lymphoma (splenic lymphoma with villous lymphocytes) Hairy cell leukemia Mycosis fungoides/Sézary syndrome (CTCL) T-cell granular lymphocytic leukemia Primary cutaneous anaplastic large cell lymphoma/lymphomatoid papulosis (CD30+) Nodular lymphocyte predominant Hodgkin's lymphoma Diffuse large cell lymphoma (includes diffuse mixed cell, diffuse large cell, immunoblastic, T-cell rich large B-cell lymphoma) Burkitt lymphoma/Burkitt cell leukemia/Burkitt-like lymphoma Precursor B- or T-cell lymphoblastic lymphoma/leukemia Primary CNS lymphoma Adult T-cell leukemia/lymphoma (HTLV 1+) MCL Polymorphic posttransplantation lymphoproliferative disorder (PTLD) AIDS-related lymphoma True histiocytic lymphoma Primary effusion lymphoma Aggressive NK-cell leukemia/blastic NK-cell lymphoma B- or T-cell prolymphocytic leukemia Key Point In addition to classifying NHL according to its cellular origin (B cell, T cell, or NK cell), it is also classified by disease course, which can be indolent or aggressive. Background An indolent disease course represents a low-grade or slow-growing malignancy. Aggressive disease states are typically characterized by intermediate and high-grade or fast-growing malignancies. As you can see in the different groupings, FL falls into the indolent category, whereas DLBCL and MCL demonstrate more aggressive courses of disease. References 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; 2008. 2. Jakić-Razumović et al. Croat Med J. 2002;43: CTCL=cutaneous T-cell lymphoma; CNS=central nervous system. Jakić-Razumović et al. Croat Med J. 2002;43: ; DeVita et al, eds. Cancer Principles and Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2008.
 CLL/SLL. LL (Waldenström’s macroglobulinemia) Extranodal marginal zone B-cell lymphoma (MALT lymphoma) Nodal marginal zone B-cell lymphoma (monocytoid B-cell lymphoma) Splenic marginal zone lymphoma (splenic lymphoma with villous lymphocytes) Hairy cell leukemia. Mycosis fungoides/Sézary syndrome (CTCL) T-cell granular lymphocytic leukemia. Primary cutaneous anaplastic large cell lymphoma/lymphomatoid papulosis (CD30+) Nodular lymphocyte predominant Hodgkin s lymphoma. Diffuse large cell lymphoma (includes diffuse mixed cell, diffuse large cell, immunoblastic, T-cell rich large B-cell lymphoma) Burkitt lymphoma/Burkitt cell leukemia/Burkitt-like lymphoma. Precursor B- or T-cell lymphoblastic lymphoma/leukemia. Primary CNS lymphoma. Adult T-cell leukemia/lymphoma (HTLV 1+) MCL. Polymorphic posttransplantation lymphoproliferative disorder (PTLD) AIDS-related lymphoma. True histiocytic lymphoma. Primary effusion lymphoma. Aggressive NK-cell leukemia/blastic NK-cell lymphoma. B- or T-cell prolymphocytic leukemia. Key Point. In addition to classifying NHL according to its cellular origin (B cell, T cell, or NK cell), it is also classified by disease course, which can be indolent or aggressive. Background. An indolent disease course represents a low-grade or slow-growing malignancy. Aggressive disease states are typically characterized by intermediate and high-grade or fast-growing malignancies. As you can see in the different groupings, FL falls into the indolent category, whereas DLBCL and MCL demonstrate more aggressive courses of disease. References. 1. Swerdlow et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. vol 2. IARC WHO Classification of Tumours, No. 2. Lyon, France: IARC Press; Jakić-Razumović et al. Croat Med J. 2002;43: CTCL=cutaneous T-cell lymphoma; CNS=central nervous system. Jakić-Razumović et al. Croat Med J. 2002;43: ; DeVita et al, eds. Cancer Principles and Practice of Oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins;2008.")
37
Non-hodgkinské lymfomy
B T null indolentní agresivní indolentní agresivní FL, CLL DLBCL MF PTCL,SS CNS

38
WHO klasifikace: indolentní B-NHL
SLL/CLL lymfoplasmocytární lymfom (imunocytom)/ W makroglobulinemie lymfomy z marginální zóny MALT Nodální (monocytoidní B) Extranodální SLVL (splenický lymfom s vilózními lymfocyty) FOLIKULÁRNÍ LYMFOM
/ W. makroglobulinemie. lymfomy z marginální zóny. MALT. Nodální (monocytoidní B) Extranodální. SLVL (splenický lymfom s vilózními lymfocyty) FOLIKULÁRNÍ LYMFOM.")
39
WHO klasifikace: agresivní B-NHL
Mantle cell lymfom (MCL) – lymfom z plášťových buněk Difuse large B cell lymphoma (DLBCL) – difuzní velkobuněčný lymfom Histol. varianty imunoblastický plasmablastický anaplastický klin. subtypy primární mediastinální primární s efuzí Burkittův lymfom Lymfoblastický lymfom
 – lymfom z plášťových buněk. Difuse large B cell lymphoma (DLBCL) – difuzní velkobuněčný lymfom. Histol. varianty. imunoblastický. plasmablastický. anaplastický. klin. subtypy. primární mediastinální. primární s efuzí. Burkittův lymfom. Lymfoblastický lymfom.")
40
WHO klasifikace NHL: T-NHL
Mycosis fungoides Periferní T lymfom (PTCL) Sézaryho syndrom Anaplastický velkobuněčný Alk1 + (T/null) Vzácné T lymfomy (hepatosplenický , angiocentrický)
 Sézaryho syndrom. Anaplastický velkobuněčný Alk1 + (T/null) Vzácné T lymfomy (hepatosplenický , angiocentrický)")
41
Časná stádia stage: I, II Pokročilá stádia: III, IV
NHL: staging Ann Arbor systém jako u HL Časná stádia stage: I, II Pokročilá stádia: III, IV

42
Monoklonální protilátky
NHL - terapie Chemoterapie Radioterapie Chirurgické řešení Monoklonální protilátky Autologní HSCT

43
NHL: přehled terapie Histologie, staging a stanovení rizikových faktorů je kruciální SLL/CLL: fludarabin + cyklofosfamid + Rituximab (anti CD20) - FCR, Folikulární lymfom: CHOP + Rituximab (R-CHOP) nebo R-COP DLBCL: CHOP + Rituximab , rizikové: eskalovaný CHOP („MegaCHOP“) nebo časově intenzifikovaný: R-CHOP 14 MCL: „Nordický protokol“´(R-CHOP + HD ARA-C + AutoHSCT) Burkittův lymfom: protokoly s vysokodávkovaným methotrexátem Lymfoblastický lymfom: jako ALL
 - FCR, Folikulární lymfom: CHOP + Rituximab (R-CHOP) nebo R-COP. DLBCL: CHOP + Rituximab , rizikové: eskalovaný CHOP („MegaCHOP ) nebo časově intenzifikovaný: R-CHOP 14. MCL: „Nordický protokol ´(R-CHOP + HD ARA-C + AutoHSCT) Burkittův lymfom: protokoly s vysokodávkovaným methotrexátem. Lymfoblastický lymfom: jako ALL.")
44
NHL: přehled terapie II
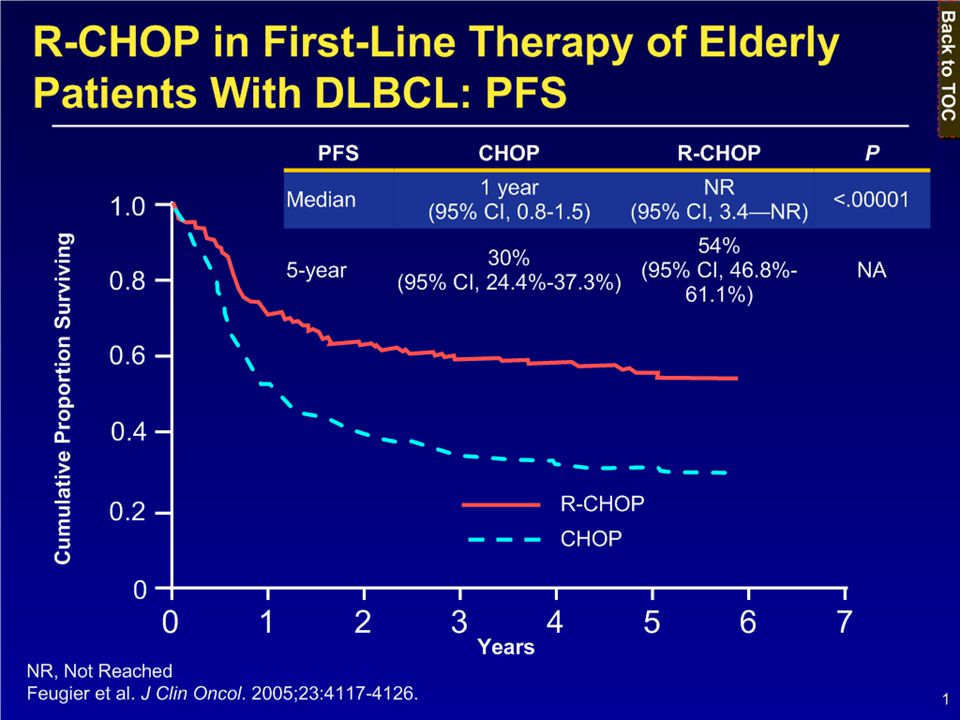
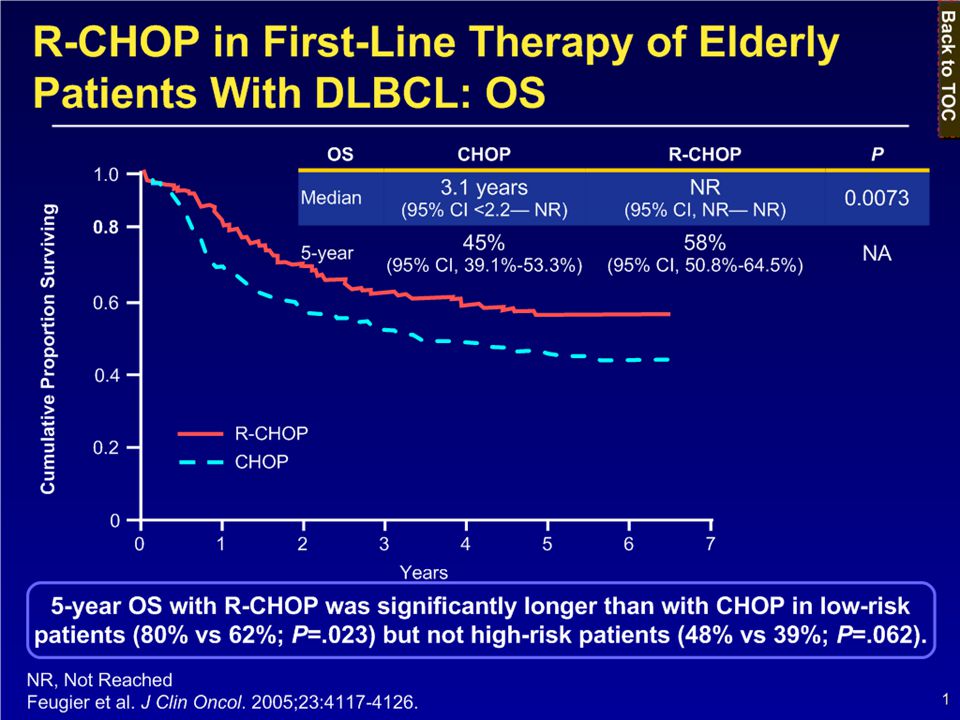
CHOP: Cyklofosfamid, Adriamycin, Vincristin, Prednison Rituximab: monoklonální protilátka anti - CD20 Prognóza: různá, záleží na histol. Subtypu a rizikových faktorech 70% pacientů s DLBCL a nízkým rizikem přežívají 5 let 20% pacientů s DLBCL a vysokým rizikem přežívají 5 let Relaps DLBCL: R- ESHAP + autologní HSCT

45
Monoklonálníprotilátky v terapii hematologických malignit
Rituximab (MabThera®) antiCD chim. Ofatumumab antiCD hum. Alemtuzumab (MabCampath®) antiCD52 hum. Y-90 Ibritumomab Tiuxetan antiCD chim. (Zevalin®) labeled Gemtuzumab ozogamicin antiCD hum. conjug. (Mylotarg®)
 antiCD20 chim. Ofatumumab antiCD20 hum. Alemtuzumab (MabCampath®) antiCD52 hum. Y-90 Ibritumomab Tiuxetan antiCD20 chim. (Zevalin®) labeled. Gemtuzumab ozogamicin antiCD33 hum. conjug. (Mylotarg®)")
46
Antigen CD20 Hydrofobní fosfoprotein, ~35kd, 167 AMK
Cytoplasma Hydrofobní fosfoprotein, ~35kd, 167 AMK Přítomen u 93% B-NHL Funkce: Ca kanál + účastní se buněčného cyklu Ne u časných prekurzorů (pro-B) a plasmatických buněk Ref. Einfeld, D.A. 7(3) EMBO Journal 711 (1988) LC1
 a plasmatických buněk. Ref. Einfeld, D.A. 7(3) EMBO Journal 711 (1988) LC1.")
47
Rituximab (anti-CD20): struktura
: struktura")
48
Přežití po zavedení Rituximabu do terapie – populační studie
2leté celkové přežití Pre Post 53% 77% <60 y 69% 87% >60 y 40% 67% Vše statisticky významné LH Sehn, ASH 2003 Abst. 88

49
Neoznačená protilátka Aboznačená radioizotopem
Radioimunoterapie Neoznačená protilátka Aboznačená radioizotopem The cytotoxic effect of monoclonal antibodies may be limited by inadequate tumour penetration. For example, antibodies may not be able to penetrate into bulky or poorly vascularised tumours. In addition, monoclonal antibodies will not affect malignant cells that do not express the target antigen. RIT can overcome some of the limitations of non-radiolabelled antibody therapy. Through a crossfire effect, radiation delivered to targeted antigen-positive cells may penetrate into bulky tumours and also reach nearby antigen-negative tumour cells.1 The radioisotope 90Y is a pure beta-emitter, with a mean path length (90) of approximately 5.3 mm in soft tissue,2,3 which is equivalent to 100250 cell diameters.4,5 Beta emission induces cellular damage by the formation of free radicals in target and neighbouring cells.6 1. Illidge TM, Johnson PW. The emerging role of radioimmunotherapy in haematological malignancies. Br J Haematol 2000;108:679–688. 2. Prestwich WV, Nunes J, Kwok CS. Beta dose point kernels for radionuclides of potential use in radioimmunotherapy. J Nucl Med 1989;30:1036–1046. 3. Potamianos S, Varvarigou AD, Archimandritis SC. Radioimmunoscintigraphy and radioimmunotherapy in cancer: principles and application. Anticancer Res 2000;20:925–948. 4. Wiseman GA, White CA, Witzig TE, et al. Radioimmunotherapy of relapsed non-Hodgkin’s lymphoma with Zevalin, a 90Y-labeled anti-CD20 monoclonal antibody. Clin Cancer Res 1999;5(Suppl):3281s–3286s. 5. Zelenetz AD. Radioimmunotherapy for lymphoma. Curr Opin Oncol 1999;11:375–380. 6. Chakrabarti MC, Le N, Paik CH, et al. Prevention of radiolysis of monoclonal antibody during labeling. J Nucl Med 1996;37:1384–1388. Illidge et al. Br J Haematol 2000;108:679688
 of approximately 5.3 mm in soft tissue,2,3 which is equivalent to 100250 cell diameters.4,5. Beta emission induces cellular damage by the formation of free radicals in target and neighbouring cells Illidge TM, Johnson PW. The emerging role of radioimmunotherapy in haematological malignancies. Br J Haematol 2000;108:679– Prestwich WV, Nunes J, Kwok CS. Beta dose point kernels for radionuclides of potential use in radioimmunotherapy. J Nucl Med 1989;30:1036– Potamianos S, Varvarigou AD, Archimandritis SC. Radioimmunoscintigraphy and radioimmunotherapy in cancer: principles and application. Anticancer Res 2000;20:925– Wiseman GA, White CA, Witzig TE, et al. Radioimmunotherapy of relapsed non-Hodgkin’s lymphoma with Zevalin, a 90Y-labeled anti-CD20 monoclonal antibody. Clin Cancer Res 1999;5(Suppl):3281s–3286s. 5. Zelenetz AD. Radioimmunotherapy for lymphoma. Curr Opin Oncol 1999;11:375– Chakrabarti MC, Le N, Paik CH, et al. Prevention of radiolysis of monoclonal antibody during labeling. J Nucl Med 1996;37:1384–1388. Illidge et al. Br J Haematol 2000;108:679688.")
50
Radioimunoterapie: 90Y-Ibritumomab tiuxetan (Zevalin®)
EU

51
90Y-Ibritumomab Tiuxetan
monoklonální Ab antiCD20 podobná rituximabu Tiuxetan (MX-DTPA) navazuje 90Y Monoklon. Ab. RIT is an innovative approach to the treatment of low-grade lymphoma, combining the tumour specificity of a monoclonal antibody with the cytotoxic activity of a radioisotope.1 Zevalin® (90Y-ibritumomab tiuxetan) uses the monoclonal antibody ibritumomab– the murine antibody that is the parent of rituximab. Ibritumomab is an IgG1 kappa monoclonal antibody directed against the CD20 antigen.2 The radioisotopes 90Y or indium-111 (111In) are linked to ibritumomab by a high-affinity chelator called tiuxetan.3 Tiuxetan is strongly bound to ibritumomab through a stable, thiourea covalent bond, providing a secure chelation site for the 90Y or 111In radioisotopes.2 1. Zelenetz AD. Radioimmunotherapy for lymphoma. Curr Opin Oncol 1999;11:375–380. 2. Chinn P, Braslawsky G, White C, Hanna, N. Antibody therapy of non-Hodgkin’s B-cell lymphoma. Cancer Immunol Immunother 2003;52:257–280. 3. Zevalin® (90Y-ibritumomab tiuxetan) prescribing information. San Diego, CA, USA: IDEC Pharmaceuticals Corporation, 2002. Chelátor Beta záření 90Y radionuklid
 navazuje 90Y. Monoklon. Ab. RIT is an innovative approach to the treatment of low-grade lymphoma, combining the tumour specificity of a monoclonal antibody with the cytotoxic activity of a radioisotope.1. Zevalin® (90Y-ibritumomab tiuxetan) uses the monoclonal antibody ibritumomab– the murine antibody that is the parent of rituximab. Ibritumomab is an IgG1 kappa monoclonal antibody directed against the CD20 antigen.2. The radioisotopes 90Y or indium-111 (111In) are linked to ibritumomab by a high-affinity chelator called tiuxetan.3. Tiuxetan is strongly bound to ibritumomab through a stable, thiourea covalent bond, providing a secure chelation site for the 90Y or 111In radioisotopes Zelenetz AD. Radioimmunotherapy for lymphoma. Curr Opin Oncol 1999;11:375– Chinn P, Braslawsky G, White C, Hanna, N. Antibody therapy of non-Hodgkin’s B-cell lymphoma. Cancer Immunol Immunother 2003;52:257– Zevalin® (90Y-ibritumomab tiuxetan) prescribing information. San Diego, CA, USA: IDEC Pharmaceuticals Corporation, Chelátor. Beta záření. 90Y radionuklid.")
52
90Y-Ibritumomab Tiuxetan (Zevalin®), standardní indikace
dospělí pacienti s relapsem FL nebo FL refrakterním vůči anti CD20 Zevalin® has been approved as a safe and effective treatment option for patients with follicular NHL refractory to rituximab.1 1. Zevalin® , EU Summary of Product Characteristics (SmPC), January 2004.
, January")
53
Principy autologní transplantace krvetvorných kmenových buněk
Odběr hem. kmenových buněk Myelo(imuno)-ablační terapie Návrat kmenových buněk Kostní dřeň PBSC (mobilizace) In vitro purging?? Rozmražení Zamražení
-ablační terapie. Návrat kmenových buněk. Kostní dřeň PBSC (mobilizace) In vitro purging Rozmražení. Zamražení.")
54
Charakteristika a současné možnosti terapie
Back to TOC Agresivní NHL Charakteristika a současné možnosti terapie Key Point The next series of slides will focus on DLBCL and MCL and provide the currently recommended therapeutic options for patients with these aggressive types of lymphomas.

55
Difuzní velkobuněčný B lymfom (DLBCL)
Back to TOC Nejčastější typ agresdivního lymfomu Obvykle symptomatický s agresivním průběhem Časté extranodální postižení Dva hlavní histologické subtypy: germinal center B cell like (GCB) a non-GCB Kurabilní v 40-50% Obvykle velké buňky s jádrem větším než u makrofágů nebo endoteliálních bb, nicméně existuje značná variabilita velikosti a tvaru buněk Friedberg JW, et al. Non-Hodgkin’s lymphoma. In: DeVita VT, et al, eds. Cancer: Principles and Practice of Oncology, v2. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008: ; Friedberg JW, et al. Diffuse large B-cell lymphoma. Hematol Oncol Clin North Am. 2008; 22(5): 941–ix.
 a non-GCB. Kurabilní v 40-50% Obvykle velké buňky s jádrem větším než u makrofágů nebo endoteliálních bb, nicméně existuje značná variabilita velikosti a tvaru buněk. Friedberg JW, et al. Non-Hodgkin’s lymphoma. In: DeVita VT, et al, eds. Cancer: Principles and Practice of Oncology, v2. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008: ; Friedberg JW, et al. Diffuse large B-cell lymphoma. Hematol Oncol Clin North Am. 2008; 22(5): 941–ix.")
56
NCCN guidelines pro léčbu DLBCL první linie (USA)
Back to TOC Nonbulky (10 cm) Adverse risk factors present R-CHOP 3 cycles LRT or R-CHOP 6-8 cycles LRT Stage I, II Adverse risk factors not present R-CHOP 3 cycles LRT or R-CHOP 6-8 cycles RT Bulky (10 cm) R-CHOP 6-8 cycles LRT Key Point The NCCN recommends R-CHOP with or without LRT as first-line treatment for patients with DLBCL at all stages of disease. Background The NCCN is a nonprofit organization comprised of an alliance of 21 of the world’s leading cancer centers. This group is dedicated to improving the quality and effectiveness of care provided to patients with cancer and develops resources that provide valuable information to health care providers, including treatment guidelines. Adverse risk factors to consider when choosing therapy for patients with stage I or II disease include elevated lactate dehydrogenase (LDH), stage II disease, age >60 years, and a performance status (PS) 2. LRT should be considered in all patients with stage I or II disease. As indicated on the following slides, many patients will relapse or not respond to R-CHOP. Therefore, additional therapeutic options are needed. Reference NCCN Web site. Accessed October 16, 2009. R-CHOP 6-8 cycles or clinical trial Stage III, IV NCCN=National Comprehensive Cancer Network; LRT=localized radiotherapy. NCCN Web site. Accessed October 16, 2009.
 Adverse risk factors present. R-CHOP 3 cycles LRT. or. R-CHOP 6-8 cycles LRT. Stage I, II. Adverse risk factors not present. R-CHOP 3 cycles LRT. or. R-CHOP 6-8 cycles RT. Bulky (10 cm) R-CHOP 6-8 cycles LRT. Key Point. The NCCN recommends R-CHOP with or without LRT as first-line treatment for patients with DLBCL at all stages of disease. Background. The NCCN is a nonprofit organization comprised of an alliance of 21 of the world’s leading cancer centers. This group is dedicated to improving the quality and effectiveness of care provided to patients with cancer and develops resources that provide valuable information to health care providers, including treatment guidelines. Adverse risk factors to consider when choosing therapy for patients with stage I or II disease include elevated lactate dehydrogenase (LDH), stage II disease, age >60 years, and a performance status (PS) 2. LRT should be considered in all patients with stage I or II disease. As indicated on the following slides, many patients will relapse or not respond to R-CHOP. Therefore, additional therapeutic options are needed. Reference. NCCN Web site. Accessed October 16, R-CHOP 6-8 cycles or clinical trial. Stage III, IV. NCCN=National Comprehensive Cancer Network; LRT=localized radiotherapy. NCCN Web site. Accessed October 16,")
59
NCCN guidelines proléčbu relabujícího/ refrakterního DLBCL (USA)
Back to TOC Suggested 2nd-Line Regimens DHAP R ESHAP R GDP R GemOx R ICE R miniBEAM R MINE R Candidate for High-Dose Therapy (HDT) Rel/Ref DLBCL Key Point The NCCN recommends a variety of regimens for patients with rel/ref DLBCL based on whether or not the patient is a candidate for high-dose therapy (HDT). Background Rituximab may or may not be added to many of the second-line regimens. Reference NCCN Web site. PDF/nhl.pdf. Accessed October 16, 2009. Clinical Trial Rituximab CEPP R PEPC EPOCH R Not Candidate for HDT Rel/Ref=relapsed/refractory; HDT=high-dose therapy. NCCN Web site. Accessed October 16, 2009.
 Rel/Ref DLBCL. Key Point. The NCCN recommends a variety of regimens for patients with rel/ref DLBCL based on whether or not the patient is a candidate for high-dose therapy (HDT). Background. Rituximab may or may not be added to many of the second-line regimens. Reference. NCCN Web site. PDF/nhl.pdf. Accessed October 16, Clinical Trial. Rituximab. CEPP R. PEPC. EPOCH R. Not Candidate for HDT. Rel/Ref=relapsed/refractory; HDT=high-dose therapy. NCCN Web site. Accessed October 16,")
60
Mantle Cell Lymfom (MCL) – lymfom z plášťových buněk
Back to TOC Představuje 7ˇ% lymfomů dospělých v Evropě a USA Characterizován translokací t(11,14)(q13;q32) , která vede k over-expresi cyklinu1 70%pacientů je při stanovení diagnózy již stádium IV Pochází z antigen-naivní periferní B buňky z vnitřní plášťové zóny Není kurabilní jako indolentní lymfomy, agresivní průběh Nepravidelná jádra, často se zářezem. Upostřed - histiocyt s eosinofilní granulovanou cytoplasmou – charakteristické u mnoha MCL. DeVita et al. DePinho et al, eds. Cancer: Principles and Practice of Oncology Review. 8th ed. Philadelphia, PA. Lippincott Williams & Wilkins; 2008: 2008; Accessed November 16, 2009.
(q13;q32) , která vede k over-expresi cyklinu1. 70%pacientů je při stanovení diagnózy již stádium IV. Pochází z antigen-naivní periferní B buňky z vnitřní plášťové zóny. Není kurabilní jako indolentní lymfomy, agresivní průběh. Nepravidelná jádra, často se zářezem. Upostřed - histiocyt s eosinofilní granulovanou cytoplasmou – charakteristické u mnoha MCL. DeVita et al. DePinho et al, eds. Cancer: Principles and Practice of Oncology Review. 8th ed. Philadelphia, PA. Lippincott Williams & Wilkins; 2008: 2008; Accessed November 16,")
61
NCCN guidelines pro první linii léčby MCL v USA
Back to TOC Stages I, II (localized presentation, extremely rare) CHOP R* R-HyperCVAD† R EPOCH NORDIC regimen Cladribine R [Any of the above RT] Clinical trial Key Point MCL patients typically present with advanced stages of MCL (stages III-IV). The NCCN recommends a variety of chemotherapy rituximab combinations with or without RT as first-line therapy. Background Patients presenting with stages I-II MCL show localized disease; identifying MCL at this stage is very rare. For patients with stages III-IV MCL, the NCCN recommends a variety of chemotherapy rituximab combinations with or without RT for first-line therapy. Patients who are in the leukemic phase with no evidence of adenopathy, are asymptomatic with stable adenopathy and nonbulky disease, or may show a nodular pattern have the option of observation only. Although an OS benefit has not yet been established, randomized studies of anthracycline-containing regimens have shown an improvement in PFS when patients undergo first-line consolidation therapy consisting of HDT with autologous stem cell rescue. References 1. NCCN Web site. Accessed October 2. Dreyling et al. Blood. 2005;105: Stages III, IV Observation only in highly selected cases RT=radiotherapy. *In selected older patients who cannot tolerate more intensive therapy.; †Modified HyperCVAD in patients >65 years of age. NCCN Web site. Accessed October 16, 2009.
 CHOP R* R-HyperCVAD† R EPOCH. NORDIC regimen. Cladribine R. [Any of the above RT] Clinical trial. Key Point. MCL patients typically present with advanced stages of MCL (stages III-IV). The NCCN recommends a variety of chemotherapy rituximab combinations with or without RT as first-line therapy. Background. Patients presenting with stages I-II MCL show localized disease; identifying MCL at this stage is very rare. For patients with stages III-IV MCL, the NCCN recommends a variety of chemotherapy rituximab combinations with or without RT for first-line therapy. Patients who are in the leukemic phase with no evidence of adenopathy, are asymptomatic with stable adenopathy and nonbulky disease, or may show a nodular pattern have the option of observation only. Although an OS benefit has not yet been established, randomized studies of anthracycline-containing regimens have shown an improvement in PFS when patients undergo first-line consolidation therapy consisting of HDT with autologous stem cell rescue. References. 1. NCCN Web site. Accessed October Dreyling et al. Blood. 2005;105: Stages III, IV. Observation only in highly selected cases. RT=radiotherapy. *In selected older patients who cannot tolerate more intensive therapy.; †Modified HyperCVAD in patients >65 years of age. NCCN Web site. Accessed October 16,")
Podobné prezentace



, Starostka D. (2. ), Vantuchová Y. (1. ) (1>")




 MYELOM.>")






 Spinoceluární karcinom (oblast horních 2/3 jícnu) Pohlaví: výskyt 7x více.>")



