Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Integrovaný blok mikrobiologie, patologie, infekční lékařství
infekcí CNS II (bakteriální etiologie) Jaroslava Dušková Ústav patologie 1.LF UK, Praha
 Jaroslava Dušková. Ústav patologie 1.LF UK, Praha.")
2
Interakce organismu a mikroorganismu - pojmy
Bakteriemie (transientní) Sepse/ Septikemie Pyemie Toxemie Viremie botulotox-blok cholinerg. transmise, diphteroxin (toxicita corynebakt. dána bakteriofágem) – kardiotox a perif.nn. až k paralyseoči, farynf,larynx, konč, resp. svaly(!)
 Sepse/ Septikemie. Pyemie. Toxemie. Viremie. botulotox-blok cholinerg. transmise, diphteroxin (toxicita corynebakt. dána bakteriofágem) – kardiotox a perif.nn. až k paralyseoči, farynf,larynx, konč, resp. svaly(!)")
3
Záněty v oblasti CNS nespecifické ohraničené „specifické“ neohraničené
hnisavé nehnisavé „specifické“ (=granulomatosní) ohraničené neohraničené
 ohraničené. neohraničené.")
4
Neuroimunoendokrinní regulace
CRF IL-1 neuronální spoje ACTH TNF IL-6 IL-1 n.vagus Glukokortikoidy Nadledviny Imunitní buňky

5
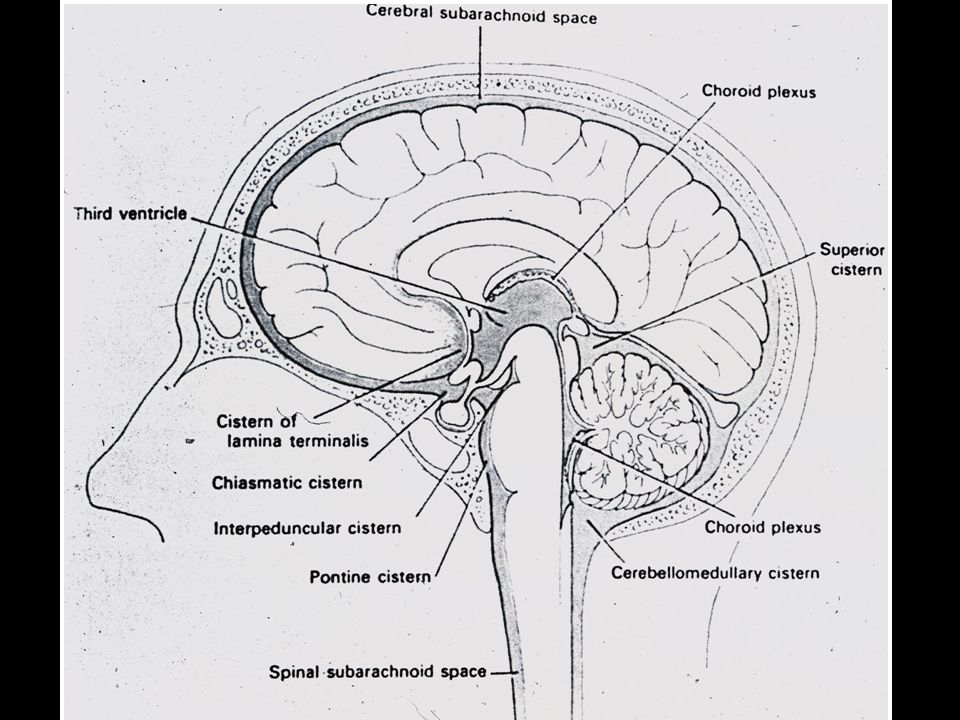
Vstup infekce do CNS hematogenní (pyemie, sepse) přímo
cestou plexus chorioideus z místního zdroje přímo (trauma) roztavením kosti (sinusitis, otitis) vv. emissariae podél nervů (filla olfactoria)
 roztavením kosti (sinusitis, otitis) vv. emissariae. podél nervů (filla olfactoria)")
6
Hematoencefalická bariera
kapilární endotelie mají těsné junkce, chybí fenestrace chudé pinocytotické vezikuly, hojné mitochondrie molekuly jsou transportovány přes endotelie pinocytozou bílé krvinky při zánětu přestupují barieru emperipolezí

8
Lymeská Borrelióza Borrelia burgdorferi (afzellii, garinii - CNS)
Ixodes ricinus „self-limited disease“ %

9
Lymeská Borrelióza Stadia 1. EM, chřipkové příznaky, lymphadenitis
2. myokarditis, vaskulitis a neurol symptomy, borreliový lymfocytom 3. chronická encephalitis, acrodermatitis chronica atrophicans (sclerodermia), arthritis
, arthritis.")
10
Fouch B, Coventry S. A case of fatal disseminated Bartonella henselae infection (cat-scratch disease) with encephalitis. Arch Pathol Lab Med Oct;131(10): cat-scratch disease / nemoc z kočičího škrábnutí Bartonella henselae inf. obvykle benigní přechodné zvětšení uzlin u imunokompetentních dětí kazuistika 6letého dosud zdravého chlapce s neobvyklou diseminací z axil. lymfadenopatie se smrtící encefalitis perivaskul. lymfocyt. infiltráty a mikrogliální uzlíky v mozku brain pcr for BH negative, positive in axillary lymhpadenopathy, extensive testing for other pathogens in brain negative, CSF serology borderline. 05/01/30 Contents | Director | Case 1 | Case 2 | Case 3 | Review 1 | EKG 1 AMR - November 2004 Case Report - A Young Woman with Cervical Lymphadenopathy Dimitrios Pappas, MD A previously healthy 34-year-old hispanic female presented to the outpatient clinic complaining of enlarged cervical lymph nodes and night sweats. She first noticed right submandibular lymph node enlargement one month prior, for which she had visited the emergency department (ED) several times and was prescribed courses of antibiotics (amoxicillin-clavulanate, ciprofloxacin, and cephalexin) without improvement. Instead, she noticed progression of the size of her lymph nodes, persistent tenderness, and development of a new palpable tender lymph node on the left side of the neck. The degree and severity of her night sweats remained unchanged. Additionally, she complained of mild fatigue. She denied loss of appetite or weight, maintained her functional baseline, and continued to work despite limitations to the range of motion of her neck due to pain. No fevers, chills, myalgias, arthralgias, changes in bowel habits or exanthems were mentioned. Furthermore, she denied vision impairment, hearing deficits or dizziness. She did not report pruritus or increased tenderness of lymph nodes following alcohol consumption. She denied dyspnea, cough, chest or abdominal pain; no abdominal fullness. She did not complain of a sore throat but admitted to mild difficulty swallowing which she attributed to the size of the lymph nodes. There was no history of tick bites, sick contacts, or recent travel; no exposure to chemicals or radiation. However, she had occupational exposure to animals and recalled a cat scratch on her forehead that had preceded the appearance of the lymphadenopathy by ten days. The patient had no significant past medical history. Her family history was significant for diabetes. She was allergic to Latex (rash). She did not smoke cigarettes or drink alcohol. Her vaccinations had been administered appropriately including booster doses for Tetanus and diphtheria. She worked in an animal shelter. On physical examination she was found to be afebrile and in no acute distress. She had a small 1 cm healing cat scratch on her forehead above the bridge of the nose. The lesion was erythematous and nontender. No conjuctivitis was noted. An obvious large (5-6 cm) right submandibular mass was present as well as a slightly smaller mass on the right anterior neck. Both sites were mildly tender, non-erythematous, and firm without surrounding cellulitis. Minimal fluctuance was detected. Her range of neck motion was decreased due to tenderness and volume of the mass. Small right preauricular lymphadenopathy was also present. No supraclavicular, axillary, epitrochlear, inguinal, or popliteal lymphadenopathy was detected. No thyromegaly was present. Cranial nerve function was normal. Vision in particular was intact and fundoscopic examination was normal. The patient had good dental hygiene without carries or oral ulcers. The trachea was midline, lung expansion was symmetric with normal resonance and breath sounds; no egophony or tactile fremitus. Heart sounds were normal, PMI was not displaced, and peripheral pulses were full and symmetric. No tenderness on palpation of the ribs or vertebrae was noted. Abdomen was soft and nontender without organomegaly or palpable masses. No peripheral edema was detected. Her skin was free of rashes or jaundice. Neurologic exam revealed no focal deficits. Laboratory data revealed a moderate leukocytosis of 12,300/mm3 (neutrophils 63% without bands, lymphocytes 24%, monocytes 9.5%, eosinophils 1%). Electrolytes and liver function tests were within normal limits. Albumin and globulin levels were normal. Lyme titer was negative. Patient also had an orthopantogram at the institution she presented initially that did not reveal any erosive or destructive lesions suggestive of an abscess. Given the history of a cat scratch, the most probable diagnosis was Cat Scratch Disease. However, persistent and progressive lymphadenopathy pointed toward the need for an immediate biopsy in order to rule out lymphoma, metastatic disease, and thyroid cancer. The fact that the lymph nodes were fluctuant and had developed over weeks was consistent with the above presumptive diagnosis. Other infections (staphylococcal and streptococcal) develop over days. Also, the absence of hard fixed nodes and the presence of fluctuance made the diagnosis of metastatic cancer less likely. At the time of the biopsy appointment, marked fluctuance was detected. Since incision for a biopsy involved the risk of an open draining wound, aspiration was recommended for pus drainage. Almost 10 ml of tan pus was aspirated and an additional lymph node biopsy was deferred. Fluid was sent for gram stain and culture. Indirect fluorescence assay (IFA) results revealed B. hensellae IgG: 4896 and B. Quintana IgG: Cultures were negative. Diagnosis was consistent with Cat scratch disease. The patient completed treatment with azithromycin. Over the next 2-3 weeks, the lymphadenopathy began to subside and almost disappeared after three months. DISCUSSION In the following section, the approach to a patient with neck lymphadenopathy will be discussed and a brief review of cat scratch disease will follow. Normal lymph nodes are usually less than 1 cm in diameter – especially when they are located in the submandibular region- and are flat and soft. There is a trend in medical practice to observe patients with a lymph node size less than 1 cm unless there are symptoms suggestive of an underlying disease. Lymphadenopathy can be caused by a vast array of diseases and drugs. In general, approximately two thirds of lymphadenopathies have nonspecific etiologies while less than 1% are due to malignancy. Distinguishing between generalized and localized lymphadenopathy, and in particular the anatomic distribution of affected lymph nodes, can guide the diagnostic approach. In the case discussed, the patient presented with localized anterior neck lymphadenopathy, which is usually attributed to upper respiratory, dental, or oral infections; rarely due to malignancies (lung, thyroid, head, and neck). Systemic infections such as infectious mononucleosis due to Epstein-Barr virus (EBV), cytomegalovirus infection (CMV), or toxoplasmosis can have a similar presentation. The texture of the lymph nodes is another characteristic that may be useful in the initial diagnostic approach. Benign lymph nodes are usually soft and movable. Tenderness is usually associated with an inflammatory process, but malignant diseases that produce rapid enlargement of the node and tension in the capsule may stimulate sensory nerve endings and also cause pain. The diagnostic workup usually involves: 1) Complete blood count that may point towards leukemias and lymphomas, or provide useful data for the diagnosis of EBV, CMV, pyogenic infections, or immune cytopenias such as systemic lupus erythematosus (SLE). 2) Serologic studies if the history is suggestive of EBV, CMV, HIV, toxoplasmosis, brucellosis, or SLE. 3) Chest X-Ray to detect the presence of pulmonary infiltrates and mediastinal lymph nodes as well as potential involvement of the lung parenchyma. 4) Other imaging techniques – CT scan, MRI, and ultrasound have been employed to differentiate between malignant and benign lymphadenopathy. 5) Biopsy: Whenever there is suspicion of malignancy based on history and clinical examination, biopsy is absolutely indicated. If history and findings suggest a benign etiology, then monitoring for 2-4 weeks is reasonable. Fine needle aspiration (FNA) should not be the first intervention and is reserved for the confirmation of cancer relapse in patients with a known primary tumor. CAT BITES Cat bites and scratches result in infection in 50% of cases. They are usually deep and sharp, and are more likely to result in septic arthritis and osteomyelitis. Pasteurella multocida is implicated in the majority of cases, although the infections are usually mixed. Rarely, it can result in the development of tetanus, the transmission of rabies or even tularemia. Cat scratch disease is a late consequence of cat bites and scratches, and bacillary angiomatosis can develop in patients with cellular immune defects. CAT SCRATCH DISEASE The microorganism responsible for the disease is Bartonella hensellae. The disease is characterized by painful regional lymphadenopathy after a cat scratch or bite. Most cases occur in children and are more common after a kitten scratch than a bite. Usually the cats are infested with fleas. It is believed that fleas transmit the responsible bacterium among cats. It is not clear whether the infection can be caused by a direct flea bite to a human. Usually after a cat scratch a local skin lesion develops – initially vesicular erythematous or papular, and then pustular. Other inoculation sites may include the eye causing conjunctivitis, and mucous membranes causing oral ulcers. The initial inoculation site may have already healed at the time the lymphadenopathy appears. After a period of 1-2 weeks tender regional lymphadenopathy develops. Occasionally, the onset may be delayed for up to 60 days and even careful inspection for possible inoculation sites may not be helpful. Since more scratches occur in the hands, the epitrochlear and axillary lymph nodes are usually involved. If the inoculation is in the conjuctiva after a cat lick then Parinaud syndrome (conjuctivitis, conjuctival granuloma, and preauricular lymphadenopathy) may develop. Parinaud sundrome may also occur after self-inoculation from another site. Neuroretinitis also may occur (optic nerve edema with macular exudates) and should be suspected in patients with fever, malaise, and blurry vision. Generalized lymphadenopathy is very rare. Involved nodes may have overlying skin erythema, and frequently become suppurative. Patients usually are otherwise asymptomatic, but systemic symptoms may develop such as fever, malaise, anorexia, and weight loss. Lymphadenopathy may persist for up to four months. Cases of cat scratch disease (CSD) lymphadenopathy persisting for 3 years have been reported. Rarely, dissemination of the infection can occur involving the CNS, bones, liver and spleen. In patients with impaired cellular immunity, such as HIV patients, bacillary angiomatosis may develop (vascular cutaneous lesions resembling Kaposi’s syndrome with possible dissemination of the infection to involve virtually every organ system). Also, the disease should be included in the differential of fever of unknown origin. The histopathology of CSD involves a granulomatous inflammation with stellate necrosis and lack of angiogenesis. In the past, skin testing was used for the diagnosis of CSD. This test involved injection of lymph node material into the skin and observing the reaction. Due to concern of transmission of viral diseases the test is not used any more. Today, the diagnosis is considered to be a clinical one. Although isolation of B. hensellae provides a definitive diagnosis it is very difficult to isolate the bacterium from tissue and most patients are not bacteremic. In addition, in terms of treatment, in vitro susceptibility does not correlate with clinical outcome. Additional testing such as the B. hensellae antibody test, Warthin-Starry stain, PCR may be used as an adjunct to the diagnosis. Available assays use the indirect fluorescence assay (IFA). However, several shortcomings interfere with the routine use of this test, such as significant cross reactivity between B. henselae and B. Quintana, suboptimal sensitivity and suboptimal specificity. IFA IgG titers <1:64 are suggestive of the absence of infection. Titers >1:256 strongly suggest active or recent infection. With intermediate titers, repeat testing in 10 to 14 days is usually recommended. The PCR test on tissue or blood is currently employed only in the research setting. Data from the current literature for treatment of CSD are obtained only from small series and case reports. The current recommendations for non life threatening CSD include a short course – 5days - of azithromycin, with alternatives including clindamycin, rifampin, trimethoprim/sulfomethoxazole, and ciprofloxacin. A combination of azithromycin with rifampin may have greater potential than either drug alone. REFERENCES 1. Spach DH, Myers SA. Cat scratch disease, UpToDate Online. Version Fletcher RH. Evaluation of peripheral lymphadenopathy in adults. UpToDate Online. Version Tompkins LS. Cat scratch disease. In: Braunwald E.(eds), et al. Harrison’s Principles of Internal Medicine. 15th Edition. McGraw Hill, 2001: pp Henry PH, Longo DL. Enlargement of lymph nodes and spleen. In: Braunwald E.(eds), et al. Harrison’s Principles of Internal Medicine. 15th Edition. McGraw Hill, 2001: pp Giladi M., Avidor B. Cat scratch disease. New England Journal of Medicine 1999;340: Bohlmann B. J., Walterspiel J. N., Giladi M., Ephros M. Treatment of cat scratch disease. New England Journal of Medicine 1999; 340: Tompkins L. S. Of cats, humans, and Bartonella. New England Journal of Medicine 1997; 337: McGill T. J.I., Wu C.-L. A 13-Year-Old Girl with a Mass in the Left Parotid Gland and Regional Lymph Nodes. New England Journal of Medicine 2002; 346:
: cat-scratch disease / nemoc z kočičího škrábnutí. Bartonella henselae inf. obvykle benigní přechodné zvětšení uzlin u imunokompetentních dětí. kazuistika 6letého dosud zdravého chlapce s neobvyklou diseminací z axil. lymfadenopatie se smrtící encefalitis. perivaskul. lymfocyt. infiltráty a mikrogliální uzlíky v mozku. brain pcr for BH negative, positive in axillary lymhpadenopathy, extensive testing for other pathogens in brain negative, CSF serology borderline. 05/01/30. Contents | Director | Case 1 | Case 2 | Case 3 | Review 1 | EKG 1. AMR - November 2004 Case Report - A Young Woman with Cervical Lymphadenopathy. Dimitrios Pappas, MD. A previously healthy 34-year-old hispanic female presented to the outpatient clinic complaining of enlarged cervical lymph nodes and night sweats. She first noticed right submandibular lymph node enlargement one month prior, for which she had visited the emergency department (ED) several times and was prescribed courses of antibiotics (amoxicillin-clavulanate, ciprofloxacin, and cephalexin) without improvement. Instead, she noticed progression of the size of her lymph nodes, persistent tenderness, and development of a new palpable tender lymph node on the left side of the neck. The degree and severity of her night sweats remained unchanged. Additionally, she complained of mild fatigue. She denied loss of appetite or weight, maintained her functional baseline, and continued to work despite limitations to the range of motion of her neck due to pain. No fevers, chills, myalgias, arthralgias, changes in bowel habits or exanthems were mentioned. Furthermore, she denied vision impairment, hearing deficits or dizziness. She did not report pruritus or increased tenderness of lymph nodes following alcohol consumption. She denied dyspnea, cough, chest or abdominal pain; no abdominal fullness. She did not complain of a sore throat but admitted to mild difficulty swallowing which she attributed to the size of the lymph nodes. There was no history of tick bites, sick contacts, or recent travel; no exposure to chemicals or radiation. However, she had occupational exposure to animals and recalled a cat scratch on her forehead that had preceded the appearance of the lymphadenopathy by ten days. The patient had no significant past medical history. Her family history was significant for diabetes. She was allergic to Latex (rash). She did not smoke cigarettes or drink alcohol. Her vaccinations had been administered appropriately including booster doses for Tetanus and diphtheria. She worked in an animal shelter. On physical examination she was found to be afebrile and in no acute distress. She had a small 1 cm healing cat scratch on her forehead above the bridge of the nose. The lesion was erythematous and nontender. No conjuctivitis was noted. An obvious large (5-6 cm) right submandibular mass was present as well as a slightly smaller mass on the right anterior neck. Both sites were mildly tender, non-erythematous, and firm without surrounding cellulitis. Minimal fluctuance was detected. Her range of neck motion was decreased due to tenderness and volume of the mass. Small right preauricular lymphadenopathy was also present. No supraclavicular, axillary, epitrochlear, inguinal, or popliteal lymphadenopathy was detected. No thyromegaly was present. Cranial nerve function was normal. Vision in particular was intact and fundoscopic examination was normal. The patient had good dental hygiene without carries or oral ulcers. The trachea was midline, lung expansion was symmetric with normal resonance and breath sounds; no egophony or tactile fremitus. Heart sounds were normal, PMI was not displaced, and peripheral pulses were full and symmetric. No tenderness on palpation of the ribs or vertebrae was noted. Abdomen was soft and nontender without organomegaly or palpable masses. No peripheral edema was detected. Her skin was free of rashes or jaundice. Neurologic exam revealed no focal deficits. Laboratory data revealed a moderate leukocytosis of 12,300/mm3 (neutrophils 63% without bands, lymphocytes 24%, monocytes 9.5%, eosinophils 1%). Electrolytes and liver function tests were within normal limits. Albumin and globulin levels were normal. Lyme titer was negative. Patient also had an orthopantogram at the institution she presented initially that did not reveal any erosive or destructive lesions suggestive of an abscess. Given the history of a cat scratch, the most probable diagnosis was Cat Scratch Disease. However, persistent and progressive lymphadenopathy pointed toward the need for an immediate biopsy in order to rule out lymphoma, metastatic disease, and thyroid cancer. The fact that the lymph nodes were fluctuant and had developed over weeks was consistent with the above presumptive diagnosis. Other infections (staphylococcal and streptococcal) develop over days. Also, the absence of hard fixed nodes and the presence of fluctuance made the diagnosis of metastatic cancer less likely. At the time of the biopsy appointment, marked fluctuance was detected. Since incision for a biopsy involved the risk of an open draining wound, aspiration was recommended for pus drainage. Almost 10 ml of tan pus was aspirated and an additional lymph node biopsy was deferred. Fluid was sent for gram stain and culture. Indirect fluorescence assay (IFA) results revealed B. hensellae IgG: 4896 and B. Quintana IgG: Cultures were negative. Diagnosis was consistent with Cat scratch disease. The patient completed treatment with azithromycin. Over the next 2-3 weeks, the lymphadenopathy began to subside and almost disappeared after three months. DISCUSSION. In the following section, the approach to a patient with neck lymphadenopathy will be discussed and a brief review of cat scratch disease will follow. Normal lymph nodes are usually less than 1 cm in diameter – especially when they are located in the submandibular region- and are flat and soft. There is a trend in medical practice to observe patients with a lymph node size less than 1 cm unless there are symptoms suggestive of an underlying disease. Lymphadenopathy can be caused by a vast array of diseases and drugs. In general, approximately two thirds of lymphadenopathies have nonspecific etiologies while less than 1% are due to malignancy. Distinguishing between generalized and localized lymphadenopathy, and in particular the anatomic distribution of affected lymph nodes, can guide the diagnostic approach. In the case discussed, the patient presented with localized anterior neck lymphadenopathy, which is usually attributed to upper respiratory, dental, or oral infections; rarely due to malignancies (lung, thyroid, head, and neck). Systemic infections such as infectious mononucleosis due to Epstein-Barr virus (EBV), cytomegalovirus infection (CMV), or toxoplasmosis can have a similar presentation. The texture of the lymph nodes is another characteristic that may be useful in the initial diagnostic approach. Benign lymph nodes are usually soft and movable. Tenderness is usually associated with an inflammatory process, but malignant diseases that produce rapid enlargement of the node and tension in the capsule may stimulate sensory nerve endings and also cause pain. The diagnostic workup usually involves: 1) Complete blood count that may point towards leukemias and lymphomas, or provide useful data for the diagnosis of EBV, CMV, pyogenic infections, or immune cytopenias such as systemic lupus erythematosus (SLE). 2) Serologic studies if the history is suggestive of EBV, CMV, HIV, toxoplasmosis, brucellosis, or SLE. 3) Chest X-Ray to detect the presence of pulmonary infiltrates and mediastinal lymph nodes as well as potential involvement of the lung parenchyma. 4) Other imaging techniques – CT scan, MRI, and ultrasound have been employed to differentiate between malignant and benign lymphadenopathy. 5) Biopsy: Whenever there is suspicion of malignancy based on history and clinical examination, biopsy is absolutely indicated. If history and findings suggest a benign etiology, then monitoring for 2-4 weeks is reasonable. Fine needle aspiration (FNA) should not be the first intervention and is reserved for the confirmation of cancer relapse in patients with a known primary tumor. CAT BITES. Cat bites and scratches result in infection in 50% of cases. They are usually deep and sharp, and are more likely to result in septic arthritis and osteomyelitis. Pasteurella multocida is implicated in the majority of cases, although the infections are usually mixed. Rarely, it can result in the development of tetanus, the transmission of rabies or even tularemia. Cat scratch disease is a late consequence of cat bites and scratches, and bacillary angiomatosis can develop in patients with cellular immune defects. CAT SCRATCH DISEASE. The microorganism responsible for the disease is Bartonella hensellae. The disease is characterized by painful regional lymphadenopathy after a cat scratch or bite. Most cases occur in children and are more common after a kitten scratch than a bite. Usually the cats are infested with fleas. It is believed that fleas transmit the responsible bacterium among cats. It is not clear whether the infection can be caused by a direct flea bite to a human. Usually after a cat scratch a local skin lesion develops – initially vesicular erythematous or papular, and then pustular. Other inoculation sites may include the eye causing conjunctivitis, and mucous membranes causing oral ulcers. The initial inoculation site may have already healed at the time the lymphadenopathy appears. After a period of 1-2 weeks tender regional lymphadenopathy develops. Occasionally, the onset may be delayed for up to 60 days and even careful inspection for possible inoculation sites may not be helpful. Since more scratches occur in the hands, the epitrochlear and axillary lymph nodes are usually involved. If the inoculation is in the conjuctiva after a cat lick then Parinaud syndrome (conjuctivitis, conjuctival granuloma, and preauricular lymphadenopathy) may develop. Parinaud sundrome may also occur after self-inoculation from another site. Neuroretinitis also may occur (optic nerve edema with macular exudates) and should be suspected in patients with fever, malaise, and blurry vision. Generalized lymphadenopathy is very rare. Involved nodes may have overlying skin erythema, and frequently become suppurative. Patients usually are otherwise asymptomatic, but systemic symptoms may develop such as fever, malaise, anorexia, and weight loss. Lymphadenopathy may persist for up to four months. Cases of cat scratch disease (CSD) lymphadenopathy persisting for 3 years have been reported. Rarely, dissemination of the infection can occur involving the CNS, bones, liver and spleen. In patients with impaired cellular immunity, such as HIV patients, bacillary angiomatosis may develop (vascular cutaneous lesions resembling Kaposi’s syndrome with possible dissemination of the infection to involve virtually every organ system). Also, the disease should be included in the differential of fever of unknown origin. The histopathology of CSD involves a granulomatous inflammation with stellate necrosis and lack of angiogenesis. In the past, skin testing was used for the diagnosis of CSD. This test involved injection of lymph node material into the skin and observing the reaction. Due to concern of transmission of viral diseases the test is not used any more. Today, the diagnosis is considered to be a clinical one. Although isolation of B. hensellae provides a definitive diagnosis it is very difficult to isolate the bacterium from tissue and most patients are not bacteremic. In addition, in terms of treatment, in vitro susceptibility does not correlate with clinical outcome. Additional testing such as the B. hensellae antibody test, Warthin-Starry stain, PCR may be used as an adjunct to the diagnosis. Available assays use the indirect fluorescence assay (IFA). However, several shortcomings interfere with the routine use of this test, such as significant cross reactivity between B. henselae and B. Quintana, suboptimal sensitivity and suboptimal specificity. IFA IgG titers <1:64 are suggestive of the absence of infection. Titers >1:256 strongly suggest active or recent infection. With intermediate titers, repeat testing in 10 to 14 days is usually recommended. The PCR test on tissue or blood is currently employed only in the research setting. Data from the current literature for treatment of CSD are obtained only from small series and case reports. The current recommendations for non life threatening CSD include a short course – 5days - of azithromycin, with alternatives including clindamycin, rifampin, trimethoprim/sulfomethoxazole, and ciprofloxacin. A combination of azithromycin with rifampin may have greater potential than either drug alone. REFERENCES. 1. Spach DH, Myers SA. Cat scratch disease, UpToDate Online. Version Fletcher RH. Evaluation of peripheral lymphadenopathy in adults. UpToDate Online. Version Tompkins LS. Cat scratch disease. In: Braunwald E.(eds), et al. Harrison’s Principles of Internal Medicine. 15th Edition. McGraw Hill, 2001: pp Henry PH, Longo DL. Enlargement of lymph nodes and spleen. In: Braunwald E.(eds), et al. Harrison’s Principles of Internal Medicine. 15th Edition. McGraw Hill, 2001: pp Giladi M., Avidor B. Cat scratch disease. New England Journal of Medicine 1999;340: Bohlmann B. J., Walterspiel J. N., Giladi M., Ephros M. Treatment of cat scratch disease. New England Journal of Medicine 1999; 340: Tompkins L. S. Of cats, humans, and Bartonella. New England Journal of Medicine 1997; 337: McGill T. J.I., Wu C.-L. A 13-Year-Old Girl with a Mass in the Left Parotid Gland and Regional Lymph Nodes. New England Journal of Medicine 2002; 346:")
Podobné prezentace

















 Mgr. Martin Šmíd.>")

 Nespecifická : Fagocytóza granulocytů,monocytů.>")