Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Aleš Tomek Neurology Department 2nd Medical Faculty of Charles University and University Hospital Motol Cerebrovascular Section of Czech Neurologic Society

2
Detection patient or bystander recognition of stroke signs, symptoms (FAST) and severity Dispatch and delivery immediate activation of EMS and prompt triage and transport to Stroke center/Comprehensive Stroke center Diagnosis + drugs/devices Recanalization th. – thrombolysis, endovascular … Disposition timely admission to neurointensive care unit Stroke recurrence prevention Detailed diagnostic of etiology and adequate prevention Disability physiotherapy incl. speech th., dysphagia th., ergotherapy, social services

3
NNT 2 NNT 7 (3,1) NNT 14 Saver JL. Stroke 2006;37(1):263-6. Hacke W et al. NEJMN 2008;359:131729. Every 1 minute will die: 1 900 000 neurons 14 000 000 000 synapses 12 km myelinated nerve fibres 90 minutes 180 minutes 270 minutes

4
Stroke ready hospital (24/365) Dedicated stroke team and equipment ▪ Cerebrovascular neurologist, neurosurgeon, neurointensivist, neuroradiologist, neurointerventionalist, physiotherapy Stroke protocols and quality of care control AIMS – to reduce mortality and morbidity: -shortening door to treatment time -increasing rates of recanalization therapy -Increasing rates of ICU hospitalized patients AIMS – to reduce mortality and morbidity: -shortening door to treatment time -increasing rates of recanalization therapy -Increasing rates of ICU hospitalized patients
 Dedicated stroke team and equipment ▪ Cerebrovascular neurologist, neurosurgeon, neurointensivist, neuroradiologist, neurointerventionalist, physiotherapy Stroke protocols and quality of care control AIMS – to reduce mortality and morbidity: -shortening door to treatment time -increasing rates of recanalization therapy -Increasing rates of ICU hospitalized patients AIMS – to reduce mortality and morbidity: -shortening door to treatment time -increasing rates of recanalization therapy -Increasing rates of ICU hospitalized patients")
5
EBM level I: SC compared to a general ward 18% relative reduction of mortality and dependent patients 3% absolute reduction in mortality = NNT 33 6% absolute increase in patients without functional deficit (mRS 0-2) = NNT 16 Stroke Unit Trialists, Cochrane Database Syst Rev 2007;(4):CD000197.
 = NNT 16 Stroke Unit Trialists, Cochrane Database Syst Rev 2007;(4):CD")
6
Canadian Stroke Network study (n = 6223) Comparing ischemic stroke mortality in stroke center vs. standard wards Lacunar stroke - 3,0 x 5,3% = OR death 0,48 Large vessel disease 7,5% x 14,5% = OR death 0,39 Cardioembolic 15,3% x 23,3% = OR death 0,46 Other causes of stroke 8,9% x 15,9% = OR death 0,45 Saposnik G et al. Int J Stroke 2011. 6(3):244-50.
:")
7
Before 2001 – without central accreditation of SC 2001 - 2009 – Stroke centers accredited only by scientific society 2010 – New system of SC/CSC – accredited by Ministry of Health + scientific societies, operational from 1. 1. 2011 11 comprehensive stroke centers 34 stroke centers From 1. 1. 2013 Quality of care indicators (every 6 months) Compulsory triage for emergency services
 Compulsory triage for emergency services.")
8
STROKE CENTER (IKTOVÉ CENTRUM) NICU – 8 beds Neurology – 30 beds Early PT – 30 beds Catchment area 400 000 inhabitants COMPREHENSIVE STROKE CENTER (KOMPLEXNÍ CEREBROVASKULÁRNÍ CENTRUM) NICU – 13 beds Neurology – 30 beds Neurosurgery – 20 beds Early PT – 20 beds Catchment area 800 000 inhabitants
 NICU – 8 beds Neurology – 30 beds Early PT – 30 beds Catchment area inhabitants COMPREHENSIVE STROKE CENTER (KOMPLEXNÍ CEREBROVASKULÁRNÍ CENTRUM) NICU – 13 beds Neurology – 30 beds Neurosurgery – 20 beds Early PT – 20 beds Catchment area inhabitants")
9
Soláň 13. - 14. 1. 2012 Ústecký kraj Ústí n. Labem Chomutov Děčín Teplice Nem. Litoměřice Liberecký kraj KN Liberec Česká Lípa Jihočeský kraj I. Nemocnice Č. Budějovice II. Nemocnice Písek Královéhradecký kraj FN Hradec Králové Obl.nem.Trutnov Obl. Nem. Náchod Jihomoravský kraj FNUSA + FN Brno Břeclav Znojmo Vyškov Moravskoslezský kraj FN Ostrava MN Ostrava Vítkovická nemocnice Krnov Třinec Karviná Olomoucký kraj IFN Olomouc Prostějov Hl. m. Praha Nemocnice Na Homolce ÚVN FN Motol VFN FNKV + FTNsP Plzeňský kraj I. FN Plzeň Karlovarský kraj Nem. Sokolov Nem. Karlovy Vary Zlínský kraj Zlín (T. Bati) Uh. Hradiště Kraj Vysočina Jihlava Nové Město na Moravě Středočeský kraj Kolín Kladno Mladá Boleslav Příbram Pardubický kraj Pardubice Litomyšl Situation 2014
 Uh. Hradiště Kraj Vysočina Jihlava Nové Město na Moravě Středočeský kraj Kolín Kladno Mladá Boleslav Příbram Pardubický kraj Pardubice Litomyšl Situation")
10
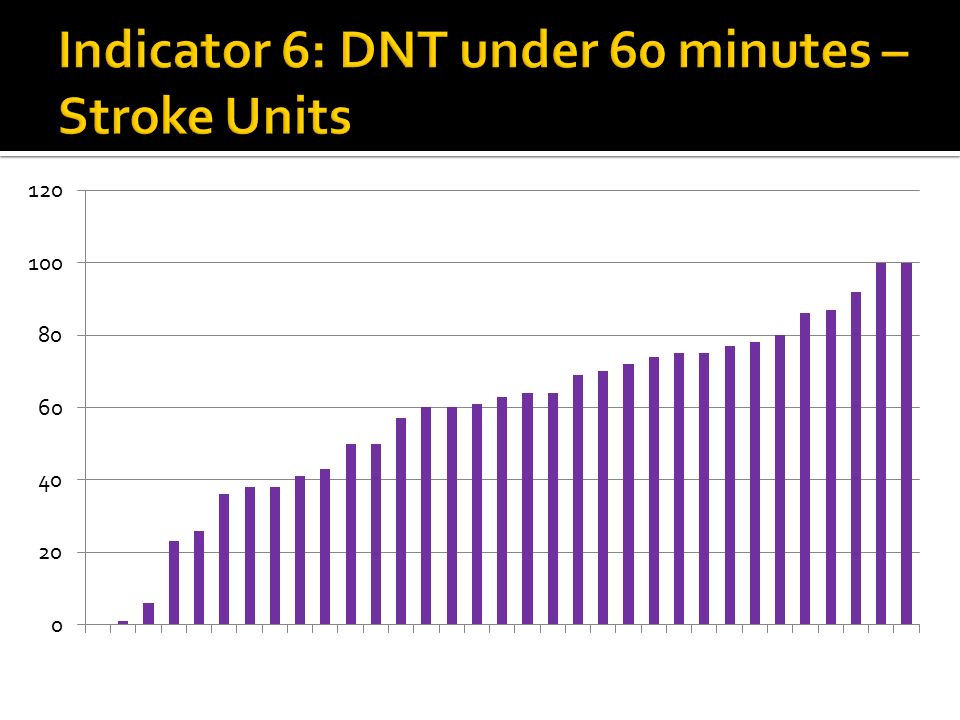
12 compulsory biannual indicators – defined by Ministry of Health and scientific societies 1x Emergency medical services – rejected admission 3x Stroke epidemiology/coverage of care ▪ Center admission– 2x – primary and secondary catchment area ▪ Mortality – 1x ▪ Length of stay – 1x 3x Recanalization therapy ▪ % IVT, DTN time <60, % endovascular 1x Rehabilitation/PT admissions 3x Neuroradiology/neurosurgery ▪ Brain vascular surgery/interventions, cerebral vessels CAS/CEA

11
I. – VI. 2013 VII. – XII. 2013

12
I. – VI. 2013VII. – XII. 2013

13
Mean I.-VI. 2013 10,54%... Mean VII.-XII. 2013 10,86% PA BV KL BK MB LTMš

14
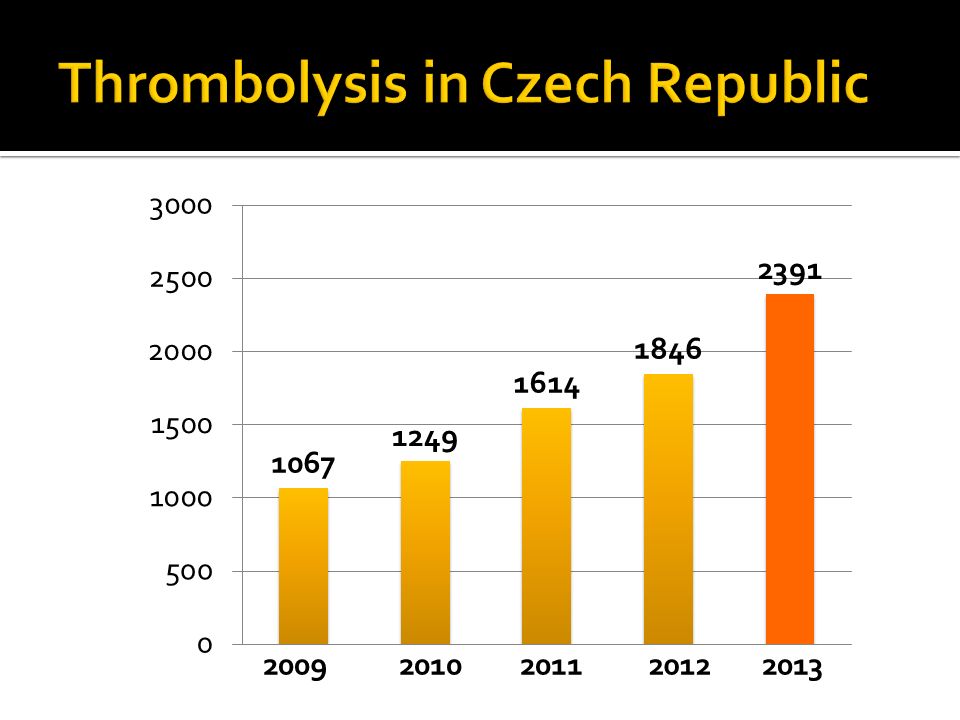
20092010201120122013
15
I. – VI. 2013 VII. – XII. 2013

17
Orange – 1 st half 2013Blue – 2 nd half 2013

18
I. – VI. 2013VII. – XII. 2013

19
VII.-XII. 2013

20
The system of care was successfully launched and is having results Compulsory quality of care indicators beneficial even after 1 year Triage of emergency medical services leads to higher admittance level to stroke units = better coverage of stroke care Indicators covering also treatment effectiveness (mortality/morbidity) not just coverage would be reasonable
 not just coverage would be reasonable")
Podobné prezentace


















 Aleš Tomek Neurologická klinika 2. LF UK a FN Motol, Praha CMP.>")
