Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Anaemia

2
Anaemia – from greek meaning ¨lack of blood¨
Anaemia= less than the normal quantity of hemoglobin in the blood Anaemic syndrome =clinical syndrome caused by tissue hypoxia

3
NORMAL VALUES OF RED BLOOD CELLS
men women Haemoglobin (Hb) – g/l Haematocrite (HTK) 0,38 – 0, ,35 – 0,46 No of erythrocytes (RBC) ,2 – 5, ,8 – 5,2 x1012/l Volume of erythrocyte (MCV) – 95 fl Mass of Hb in erythrocyte – 32 pg (MCH) Hb concentration in erythrocyte ,32 – 0,37 (MCHC)
 136 – g/l. Haematocrite (HTK) 0,38 – 0,49 0,35 – 0,46. No of erythrocytes (RBC) 4,2 – 5,8 3,8 – 5,2 x1012/l. Volume of erythrocyte (MCV) 80 – 95 fl. Mass of Hb in erythrocyte 26 – 32 pg. (MCH) Hb concentration in erythrocyte 0,32 – 0,37. (MCHC)")
4
NORMAL VALUES OF RED BLOOD CELLS
men women Haemoglobin (Hb) – g/l Haematocrite (HTK) 0,38 – 0, ,35 – 0,46 No of erythrocytes (RBC) 4,2 – 5, ,8 – 5,2 x1012/l Volume of erythrocyte (MCV) – 95 fl Mass of Hb in erythrocyte – 32 pg (MCH) Concentration of Hb in erythrocyte ,32 – 0,37 (MCHC)
 136 – g/l. Haematocrite (HTK) 0,38 – 0,49 0,35 – 0,46. No of erythrocytes (RBC) 4,2 – 5,8 3,8 – 5,2 x1012/l. Volume of erythrocyte (MCV) 80 – 95 fl. Mass of Hb in erythrocyte 26 – 32 pg. (MCH) Concentration of Hb in erythrocyte 0,32 – 0,37. (MCHC)")
5
Anaemic syndrome - symptoms rom (AS)
Tissue hypoxia: pallor, fatigue, weakness, dyspnea Compensation and adaptation: Hypercinetic circulation, palpitations, tinnitus Secondary : Cardiovascular symptoms – decompensation of ischemic heart disease, AP, IM, claudications…

6
Anemický syndrom (AS) Progress and severity of AS depends on:
1. Absolute value of Hb Hgb g/l = most of patients suffer from symptoms 2. Speed of onset 3. Age and overall performance of the patient

8
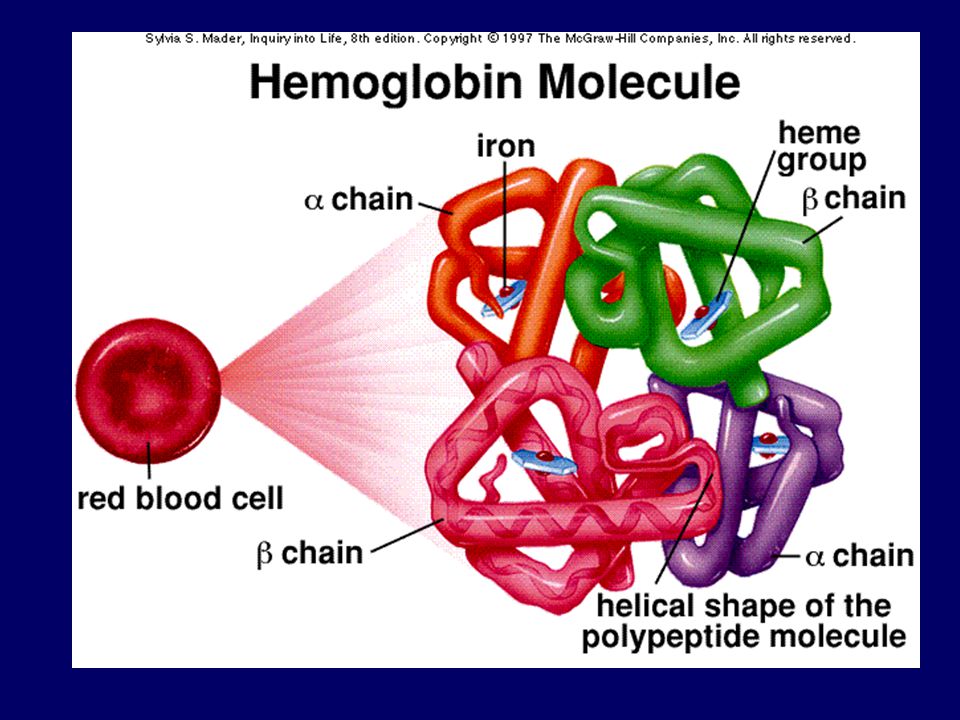
HAEM + GLOBIN HAEMOGLOBIN DNA – B12 ,folic acid, EPO
IRON PROTOPORFYRIN HAEM GLOBIN HAEMOGLOBIN DNA – B12 ,folic acid, EPO

9
ANAEMIA - CLASSIFICATION
Morfologic criteria: According to MCV: (80 – 95 fl) microcytic, normocytic, macrocytic According to MCH: (27-32 pg) normochrome, hypochrome According to no of reticulocytes: (0,7 – 2,8 %) anaemia with lowered, normal or incresed no of reticulocytes
 microcytic, normocytic, macrocytic. According to MCH: (27-32 pg) normochrome, hypochrome. According to no of reticulocytes: (0,7 – 2,8 %) anaemia with lowered, normal or incresed no of reticulocytes.")
10
Iron deficiency anaemia Chronic disease anaemia
MICROCYTIC ANAEMIA Iron deficiency anaemia Chronic disease anaemia Thalasemia, sideroblastic anaemia MACROCYTIC ANAEMIA Megaloblaste anaemia(lack of B12, folic acid, MDS) Macrocytic non-megaloblaste anaemia (usually secondary) NORMOCYTIC ANAEMIA Primar impairment of blood marrow: aplastic anaemia, MDS, PNH, myelofibrosis. Secondary impairment of blood marrow :(infiltration, infection, endocrinological and systemic diseases, ACD) D. ANAEMIA WITH RETICULOSIS Haemolytic aneamia corpuscular Haemolytic anaemia extracorpuscular – imunne and non-immune based
 Macrocytic non-megaloblaste anaemia (usually secondary) NORMOCYTIC ANAEMIA. Primar impairment of blood marrow: aplastic anaemia, MDS, PNH, myelofibrosis. Secondary impairment of blood marrow :(infiltration, infection, endocrinological and systemic diseases, ACD) D. ANAEMIA WITH RETICULOSIS. Haemolytic aneamia corpuscular. Haemolytic anaemia extracorpuscular – imunne and non-immune based.")
11
Pathofysiological classification

12
EPO

13
EPO TSH Fe, Fol, B12 C, E

17
Pathofysiological classification
Proliferation and differentiation disorder Increased destruction of RBC Blood loss Combined etiology

18
HEM + GLOBIN thalasemia HEMOGLOBIN DNA – B12, folic acid, EPO
IRON PROTOPORFYRIN Iron insufficiency sideroblastic anaemia ACD HEM GLOBIN thalasemia HEMOGLOBIN DNA – B12, folic acid, EPO

19
Iron defficiency

20
Iron defficiency Most frequent cause of anemia
( worldwide – WHO) 80%of all anaemia SA: 10% of fertile women Sideropenia: 35-58% of fertile women
 80%of all anaemia. SA: 10% of fertile women. Sideropenia: 35-58% of fertile women.")
21
Iron defficiency CAVE: influencing not just the blod count!
DNA synthesis impairement Tissue fosforylation impairement Purine metabolism impairement Colagen synthesis impairement Granulocyte function impairement Neurotransmiter function impairement

22
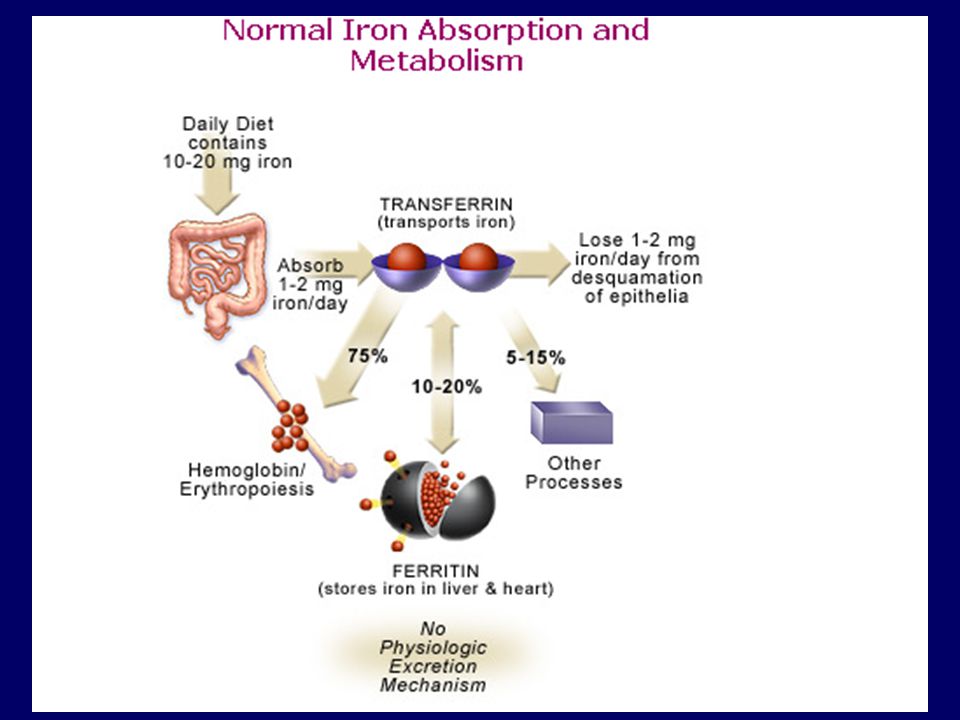
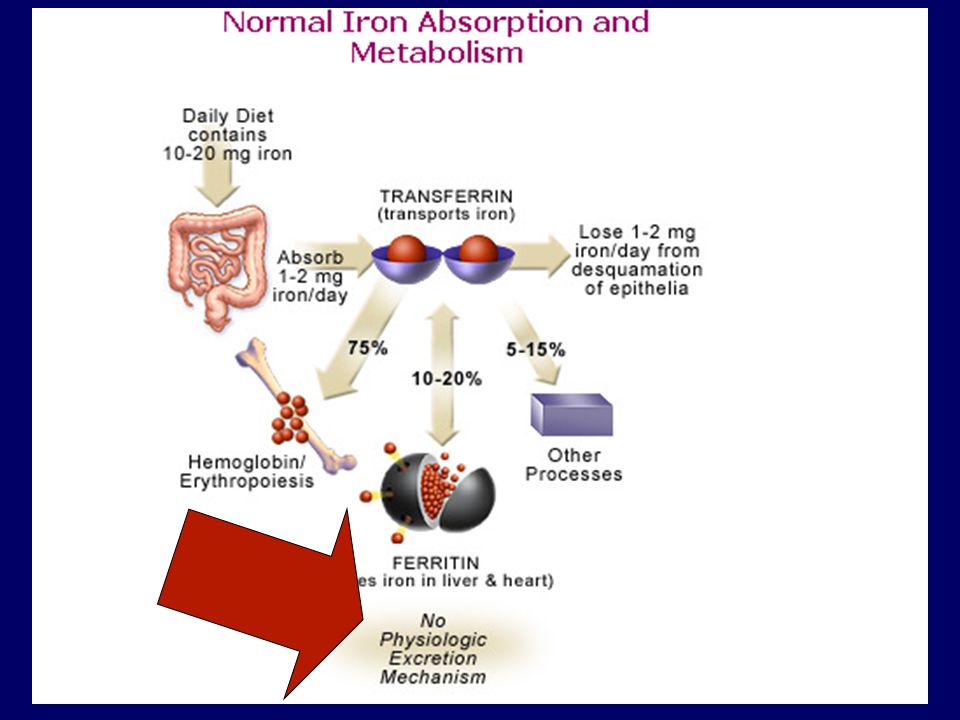
Iron distribution in the organism

25
Iron metabolism Food contents: 15-20mg/den
Absorption: 1-2mg (duodenum, upper part of jejunum) Loss (epitel desqvamation) 1-2mg Pregnancy: overall loss: mg Supply in the organism: mg
 Loss (epitel desqvamation) 1-2mg. Pregnancy: overall loss: mg. Supply in the organism: mg.")
26
Hepcidine Acute phase reactant Source: hepatic cells, heart,
Iron stimulates Hepcidine Hepcidine inhibits iron absorption in the intestine, iron release from macrophages and iron transport via placenta ACD, hereditary hemochromatosis

27
Iron defficiency Insufficient intake - malnutrition
Absorption impairement – maldigestion, malabsorption Increased loss Lowered intake

28
Insufficient intake Malnutrition Imbalanced diet Vegetarians
- Meat: 25-30% of iron is absorbed - Vegetables: 5% of iron is absorbed

29
Iron absorption from various foods (%)
Rice Spinach Beans Corn Lettuce Wheat Soya Ferritin Veal liver Fish meat Haemoglobin Veal meat

30
Rice Spinach Beans Corn Lettuce Wheat Soya beans Ferritin Veal liver
Iron absorption from various foods (%) Rice Spinach Beans Corn Lettuce Wheat Soya beans Ferritin Veal liver Fish meat Haemoglobin Veal meat
 Rice. Spinach. Beans. Corn. Lettuce. Wheat. Soya beans. Ferritin. Veal liver. Fish meat. Haemoglobin. Veal meat.")
31
Resection of stomach – 65% patients Achlorhydria Coeliakia M. Crohn
Absorption disorder Resection of stomach – 65% patients Achlorhydria Coeliakia M. Crohn Infection H. Pylori with gastritis

32
Loss GIT (h. hernia, gastritis, ulcerous disease, tumours, intestinal inflammmatory diseases, hemorhoids, parasites, diverticulitis…) Respiratory tractus Urogenital tract Menses = cca 3mg Fe / den NSAIDs, hemodialysis, blood testing, self - harming

33
Increased need Gravidity Brest-feeding Growth

34
Symptoms Anemic syndrome Cefalea, paresthesia, fatigue
Tongue burning, angulitis Odyno-, dysfagia Sy Kelly-Patterson Brittle hair, nails (Pica, pagofagia)
")
35
Physical examination Pallor – skin, mucous membrane Blue sclerae
Ulcers/ angulitis Smooth tongue Straight/(spoon-shaped) nails Achlorhydria, atrophic gastritis
 nails. Achlorhydria, atrophic gastritis.")
36
Laboratory findings RDW: high Trombocytosis (over 50% of patients)
BM –staining for iron - lack of Fe in siderophages - sideroblasts lower then 10%

37
Laboratory findings MCV under 80fl MCH under 25ug MCHC – late symptom
Transferrin -increased S-ferritin <20ug/l Transferrin satur. – under15 % (N: 20-40%) VKFe (TIBC): increased S-sTfR > 8g/l
 VKFe (TIBC): increased. S-sTfR > 8g/l.")
38
DIFFERENTIAL DIAGNOSIS OF IRON INSUFFICIENCY (mikrocytic anaemia)
Fe TIBC satTRF ferritin TRF receptor _______________________________________________ Iron insuf Chronic disease associated anaemia N N N (ACD) Thalasemia N or N or N or N or
 Thalasemia N or N or N or N or ")
39
CAVE Ferritine Acute phase reactant Nespecific tumorous marker
Level increases with age (75ug/l in old people = ? = iron defficiency)
")
40
Iron defficiency Prelatent Latent Manifest - SA

41
Typical patient with IDA
Woman 20-45y, fatigue, sleepiness, ear buzzing, hairloss, brittle nails, hyper- polymenorhea or normal menses. 2. Man 50y or older, dysfagia, weightloss, treated with ASA for ICD, blood in stools or urine.

42
= Treatment of the cause of iron loss + iron supply
Treatment of IDA = Treatment of the cause of iron loss + iron supply

44
Ferrotherapy 150-200mg Fe / day
Until enough supply is formed (ferritin 50ug/l) Use on an empty stomach CAVE: polyphenols, milk, egg yolk Dyspepsia Parenteral forms (CAVE: anaphylaxis; x new forms are safer - karboxymaltose)
 Use on an empty stomach. CAVE: polyphenols, milk, egg yolk. Dyspepsia. Parenteral forms (CAVE: anaphylaxis; x new forms are safer - karboxymaltose)")
45
PŘÍPRAVKY ŽELEZA tab název léková složení obsah látky v lékové
(výrobce) forma formě Aktiferrin cps. síran železnatý 34 mg (Merckle,SRN) serin sir. 6,8 mg/ml gtt. 9,3 mg/ml Ferrlecit inj komplex Fe 3+ s glukonátem 62,5 mg (Nattermann,SRN) sodným Ferro-Gradumet 105 mg (Galenika,Jugoslávie) Ferronat susp. fumarát železnatý 10 mg/ml (Galena,ČR) Ferronat retard (Léčiva,ČR) Ferrum lek i.m. komplex hydroxidu 100 mg (Lek,Slovinsko) železitého se sacharózou Maltofer (Vifor,Švýcarsko) s polymaltosou 50 mg/ml Sorbifer durules (Egis,Maďarsko) kyselina askorbová Tardyferon drg 80 mg (Robapharm,Švýcarsko) mukoproteáza Ferinject (Vifor, Francie) inj Fe3+ karboxymaltóza mg, 500mg
 forma. formě. Aktiferrin. cps. síran železnatý. 34 mg. (Merckle,SRN) serin. sir. 6,8 mg/ml. gtt. 9,3 mg/ml. Ferrlecit. inj. komplex Fe. 3+ s glukonátem. 62,5 mg. (Nattermann,SRN) sodným. Ferro-Gradumet. 105 mg. (Galenika,Jugoslávie) Ferronat. susp. fumarát železnatý. 10 mg/ml. (Galena,ČR) Ferronat retard. (Léčiva,ČR) Ferrum lek i.m. komplex hydroxidu. 100 mg. (Lek,Slovinsko) železitého se sacharózou. Maltofer. (Vifor,Švýcarsko) s polymaltosou. 50 mg/ml. Sorbifer durules. (Egis,Maďarsko) kyselina askorbová. Tardyferon. drg. 80 mg. (Robapharm,Švýcarsko) mukoproteáza. Ferinject (Vifor, Francie) inj. Fe3+ karboxymaltóza 100mg, 500mg.")
46
P.o. iron treatment control
Reticulocyte crisis D 10-14 Increase of haemoglobin Normalisation of MCV a RDW Iron supply forming Ineffective treatment: Diagnosis checking :BM examination, GIT examination aso…. Cave self-harming Switch to i.v. therapy

47
Thalassemia

48
IRON PROTOPORFYRIN HEM + GLOBIN HEMOGLOBIN DNA – B12 , folic acid
Fe insufficiency sideroblastic anemia ACD HEM GLOBIN thalasemia HEMOGLOBIN DNA – B12 , folic acid

49
Thalassemia + thalasemia, 0thalasemia Fetus: - Hb F α2 γ2
Adult - Hgb A: α2 β2 - Hgb A2: α2 δ2 - Hgb F: α2 γ2

50
Thalassemia α –thalasemia = α disorder β – thalasemia = β disorder

51
α - Thalassemia (Normal genotype: α α / α α) - α/ α α = silent carrier
- α/- α , - - / α α = carrier (mikrocytosis, erythrocytosis): = Thalassemia minor - - / - α = HbH (β4) (splenomegalia, mikrocytosis, bones) - - / - - = hydrops fetalis, sy Hb Bart´s (γ4)
: = Thalassemia minor. - - / - α = HbH (β4) (splenomegalia, mikrocytosis, bones) - - / - - = hydrops fetalis, sy Hb Bart´s (γ4)")
52
β - Thalassemia More severe then α–thalassemia
β – thalasemia minor (β+/ β, β0/ β) Mikrocytosis, anaemia, erythrocytosis β – thalasemia intermedia (β+/ β+, β0/ β+) β – thalasemia major (β0/ β0, β+/ β+) Severe anemia, anisopoikilocytosis, affected ERY, HbF, hepatosplenomegalia,bone deformities,permanent transfusion therapy, Fe overload, Tx, splenectomia, HU
 Mikrocytosis, anaemia, erythrocytosis. β – thalasemia intermedia (β+/ β+, β0/ β+) β – thalasemia major (β0/ β0, β+/ β+) Severe anemia, anisopoikilocytosis, affected ERY, HbF, hepatosplenomegalia,bone deformities,permanent transfusion therapy, Fe overload, Tx, splenectomia, HU.")
53
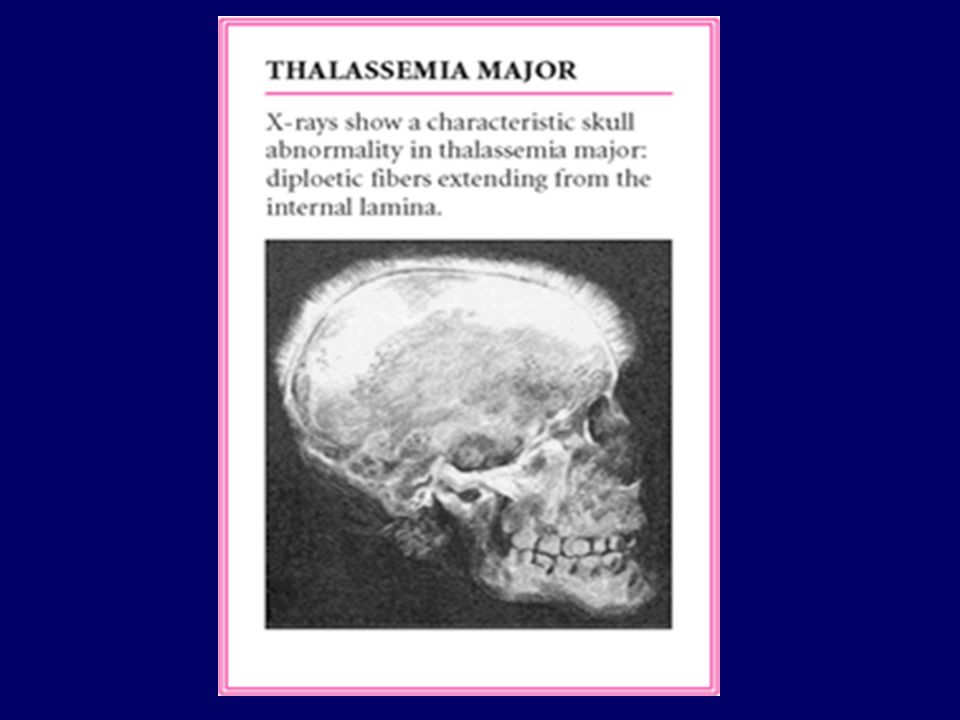
BETA THALASEMIA Pathogenesis:
chains formation impairement increased synthesis of and Alpha chains overdose –low solubility, precipitation, agregates deform cell membranes Hb – easy autooxidation, lower stability release of Fe cell destruction by peroxidative lipid cleavage. Inefective erythropoiesis, large numbers of erytrocytes decline as soon as the BM + peripheral hemolysis + shortened lifespan Significant compensatory erythropoiesis hyperplasia corticalis usurationbone deformities, fractures, extramedular hemopoiesis Relative Fe defficiency in BM because of hyperplastic erythropoiesis, at the same time increased Fe supply (coming from destroyed ery in monocyte- macrophage system) increased Fe resorption in the intestine Fe overload of the organism (together with Fe coming from transfusions).
 increased Fe resorption in the intestine Fe overload of the organism (together with Fe coming from transfusions).")
56
MEGALOBLASTIC ANAEMIA
Lack of B12of folic acid: 1. Pernicious anaemia - B12 absorption in the distal intestine disorder due to lack of intrinsic factor (produced by parietal cells of gastric mucosa) 2. Dihydrofolat reductase inhibitors (MTX, ARA-C)
 2. Dihydrofolat reductase inhibitors (MTX, ARA-C)")
57
MEGALOBLASTIC ANAEMIA -CAUSES
Insufficient intake of B12 of folic Absorption impairement: a) lack of intrinsic factor, intrinsic factor b) celiakia, Crohn disease, intestinal resection, diverticules, strictures,parasites c) resorption inhibitors (fenylhydantoin,PAS,pyrimidin, neomycin) d) selective malabsorption B12 with proteinuria Transport disorders because of lack of transkobalamin I. and II. Increased demand (gravidity, growth, anaemia with hyperplasia of erythropoiesis Increased loss (hepatic laesions, bleeding) dihydrofolat reductase inhibitors (MTX,pyrimethamin) pyrimidin antagonists (ARA-C) / purin antagonists (6-MP)
 lack of intrinsic factor, intrinsic factor. b) celiakia, Crohn disease, intestinal resection, diverticules, strictures,parasites. c) resorption inhibitors (fenylhydantoin,PAS,pyrimidin, neomycin) d) selective malabsorption B12 with proteinuria. Transport disorders because of lack of transkobalamin I. and II. Increased demand (gravidity, growth, anaemia with hyperplasia of erythropoiesis. Increased loss (hepatic laesions, bleeding) dihydrofolat reductase inhibitors (MTX,pyrimethamin) pyrimidin antagonists (ARA-C) / purin antagonists (6-MP)")
58
Megaloblastic anaemia
Blood count– macrocytes (↑MCV, ↑MCH,normal MCHC), ↓RTC, megalocytes, megaloblasts, leukocytosis with left shift, thrombocytopenia. Bone marrow– hyperplasia of erytropoiesis, megaloblasts, granulocyte macrocytosis, mgkc. polyploidia dif.dg. MDS (cytogenetics, cytochemistry) biochemistry – ↓ B12, ↓folic acid, ↑direct and indirect bilirubin, intrinsic factor antibodies, antibodies against parietal cells, normal iron supplies
, ↓RTC, megalocytes, megaloblasts, leukocytosis with left shift, thrombocytopenia. Bone marrow– hyperplasia of erytropoiesis, megaloblasts, granulocyte macrocytosis, mgkc. polyploidia. dif.dg. MDS (cytogenetics, cytochemistry) biochemistry – ↓ B12, ↓folic acid, ↑direct and indirect. bilirubin, intrinsic factor antibodies, antibodies against parietal cells, normal iron supplies.")
60
Proteins binding VITAMIN B12
Intrinsic factor B12 absorption in ileum, binding to specific receptor (cubilin) Secerned by parietal gastric cells In case of lack leads to B12 malabsorption TRANSCOBALAMIN I Binds B12 in plasma,binds to B12 in stomach before binding to intrinsic factor, produced by neutrofiles and cells with exocrine secretion, his lack leads to low serum B12 levels TRANSCOBALAMIN II Enables B12 absorption by cells, receptor on all type of cells, produced by endotelial cells, fibroblasts, ileum cells.., his lack leads to severe B12 deficiency in cells
 Secerned by parietal gastric cells. In case of lack leads to B12 malabsorption. TRANSCOBALAMIN I. Binds B12 in plasma,binds to B12 in stomach before binding to intrinsic factor, produced by neutrofiles and cells with exocrine secretion, his lack leads to low serum B12 levels. TRANSCOBALAMIN II. Enables B12 absorption by cells, receptor on all type of cells, produced by endotelial cells, fibroblasts, ileum cells.., his lack leads to severe B12 deficiency in cells.")
62
Pernicious anaemia

63
Megaloblastic anaemia Diferential dg.:
atrofic gastritis / sprue/ inflamations, parasites/ medication/ liver laesions DNA synthesis impairement due to abnormal cell clone– MDS (bone marrow biopsy, cytogenetics, cytochemistry, B12)
")
64
Treatment Substitution - vitamin B12 300 – 1000 μg/d
- maintainance dose 1 x za 6 – 8weeks all life long reticulocyte crisis : 5.-7.d of treatment rise of reticulocyte count up to 10-30%. need of iron metabolism parameters, regular GSK and colonoscopy

65
Autoimmune disease Smooth tongue surface, vitiligo, grey hair Not just anaemia, but pancytopenia Parenteral substitution of B12 Reticulocyte crisis GSK á 1-2years

66
Anaemia with increased no of reticulocytes
HEMOLYTIC ANAEMIA - corpuscular - estracorspuscular bleeding - acute

67
CORPUSCULAR HEMOLYTIC ANAEMIA
MEMBRANE DEFECTS ENZYMOPATIA HEMOGLOBINOPATIA

68
NON-IMMUNE ACQUIRED HEMOLYTIC ANAEMIA
MECHANICAL AND PHYSICAL CAUSES heart valve impairement hemoglobinuria microangiopatic hemolytic anemia widespread burns METABOLIC CAUSES liver disease, alcoholism hypofosfatemia hereditary abetalipoproteinemia malnutrition Cu overload Wilsonś disease CHEMICAL SUBSTANCES oxidative agents, snake venon INFECTIONS Direct ery infection – malaria septicemia ( clostridium perfringens aj. ) leptospira, borelia
 leptospira, borelia.")
69
Corpuscular Haemolytic anaemias
Pathogenesis Lack of and defects in membrane proteins (ankyrin, spectrin, etc.) Decreasesd size of ery surface – spherocyte increased cell membrane permeability ( Na ) Increased need for eneregy - - (Na pump) increased rigidity and loss of flexibility passge through spleen sinusoid more difficult loss of membrane parts – microspherocyte cell deth in the spleen EXTRAVASCULAR HAEMOLYSIS
 Decreasesd size of ery surface – spherocyte. increased cell membrane permeability ( Na ) Increased need for eneregy - - (Na pump) increased rigidity and loss of flexibility. passge through spleen sinusoid more difficult loss of membrane parts – microspherocyte. cell deth in the spleen EXTRAVASCULAR HAEMOLYSIS.")
70
Hereditary spherocytosis
Autosomal dominant ( rarely recesiive) disease with variable gene expressivity variable clinical symptoms (phenotype) ( anemia with ićterus, splenomegaly, hemolytic crisis ). Diagnostics: Anemia + s reticulocytosis + spherocytes in blood smear, Hyperplůasti erythropoiesis in bone marrow, increased level of both direct and indirect bilirubin, serum Fe a feritin not increased Osmotic resistance of erythrocytes decreased Autohemolýza ( upravuje se po podání glukózy i ATP ) increased PINK test Dif dg.: other corpuscular anemias (HE, etc.) imunne hemolytic anemias non-immune extracorpuscular hemolytic anemias paroxysmal nocturnal hemoglobinuria sometimes MDS Léčba: splenectomy
 disease with variable gene expressivity variable clinical symptoms (phenotype) ( anemia with ićterus, splenomegaly, hemolytic crisis ). Diagnostics: Anemia + s reticulocytosis + spherocytes in blood smear, Hyperplůasti erythropoiesis in bone marrow, increased level of both direct and indirect bilirubin, serum Fe a feritin not increased. Osmotic resistance of erythrocytes decreased. Autohemolýza ( upravuje se po podání glukózy i ATP ) increased. PINK test. Dif dg.: other corpuscular anemias (HE, etc.) imunne hemolytic anemias. non-immune extracorpuscular hemolytic anemias. paroxysmal nocturnal hemoglobinuria. sometimes MDS. Léčba: splenectomy.")
71
ERYTROCYTE ENZYMOPATHY
Defects in enzymes of anaerobe glykolysis pyruvát kinázy defficiency (PKD) – chronic: haemolytick anemia, with little effect of splnectomia Defect in enzymes of pentos cycle glucose-6-phosphate dehydrogenase defficiency increased sensitivity to oxydazing agents – chronic haemolysis or haemolytic crisis– anemia with Heinz bodies
 – chronic: haemolytick anemia, with little effect of splnectomia. Defect in enzymes of pentos cycle. glucose-6-phosphate dehydrogenase defficiency. increased sensitivity to oxydazing. agents – chronic haemolysis. or haemolytic crisis– anemia with Heinz bodies.")
72
ANAEROBE GLYKOLYSIS

73
GLUCOSE-6-PHOSPHATE DEHYDROGENASE defficiency
Results in: lack of NADPH …. Increased sensitivity to oxydating agents Gene for G6PDH: X – chromosome , wide physiologic variability of the enzyme Mutation: mostly point mutation in 1 or to bases decreased enzyme production, production of the enzyme with decreased activity or production of the enzyme with decreased afinty to the substrate or with decreased stability Wide variability in clinical symptoms : Silent carrier severe haemolytic crisis, neonatal icterus Diagnostics: G-6-PD activity analysis Activity to substrate analysis, mobility in ELFO, stability Molecular genetics Other: GSH stability test, Heinz body formation test Th: Prevention of exposure to oxydative agents (medication: antimalarics, sulfonamides,. Food: vicia fava etc.) , splenectomy, stem cell transplant
 , splenectomy, stem cell transplant.")
76
HEMOGLOBINOPATHIES Abnormal Hb with mostly one aminoacid (AA) substitution in the globion chaine a/ sicle cell anemia – HbS b/ Hb C, Hb D, Hb E – chronic haemolytic anemias often in combination with Hb S or thal c/ instable haemoglobin diseases hydrofobe AA decreased binding activity of Hb or impaired secondary structure of Hb and contacts between subunits chronic hemolytic anemia with Heinz bodies( denaturation of nestable Hb ) d/ methemglobinemia Fe3+ stabilisation due to histidine tyrosine in proximity of hem group results in cynosis e/ hemoglobine with increased oxygen affinity tissue hypoxia, cyanosis, polycythaemia in blood count. Diagnostika: elfo Hb identifikace abnormálního Hb tryptickým štěpením isopropanol test, Heinz body tests, methemoglobine tests, afinity to O2 tests molekular genetics, DNA analysis
 d/ methemglobinemia. Fe3+ stabilisation due to histidine tyrosine in proximity of hem group results in cynosis. e/ hemoglobine with increased oxygen affinity. tissue hypoxia, cyanosis, polycythaemia in blood count. Diagnostika: elfo Hb. identifikace abnormálního Hb tryptickým štěpením. isopropanol test, Heinz body tests, methemoglobine tests, afinity to O2 tests. molekular genetics, DNA analysis.")
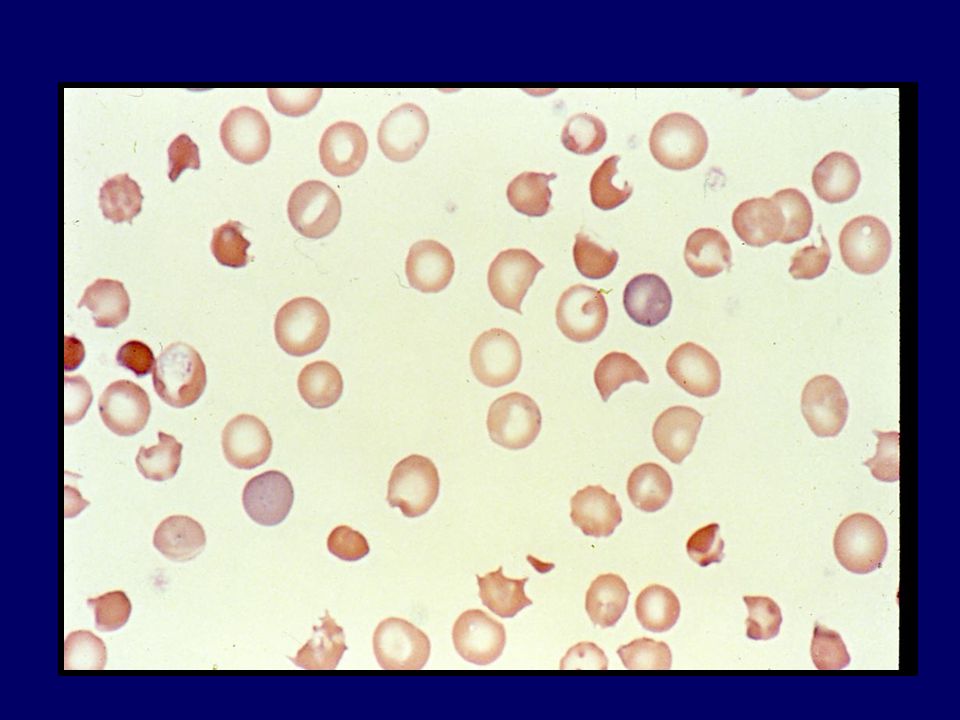
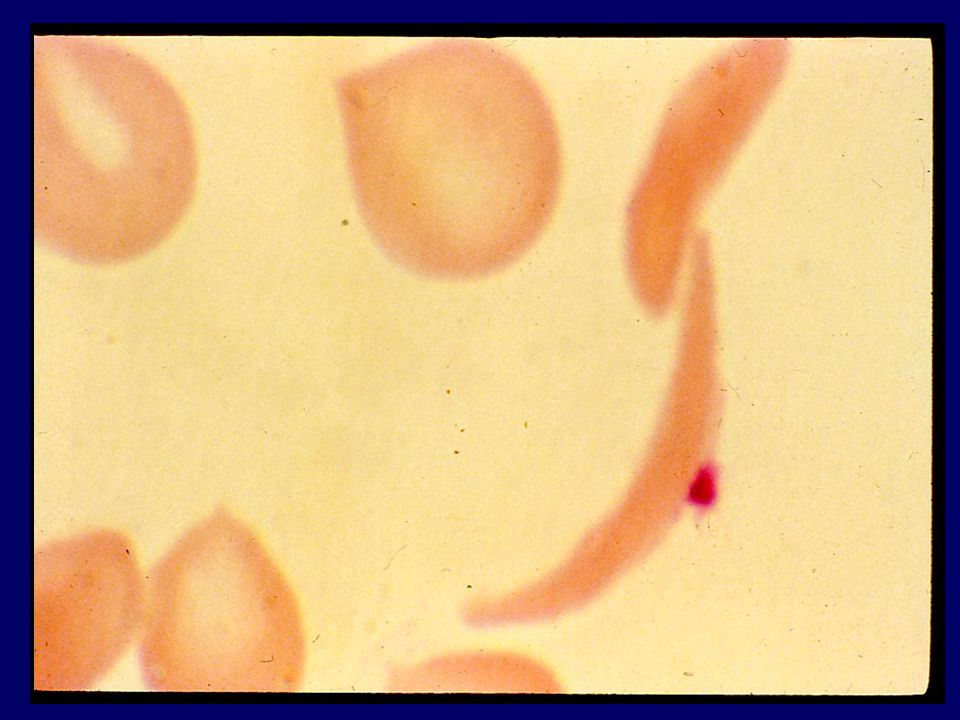
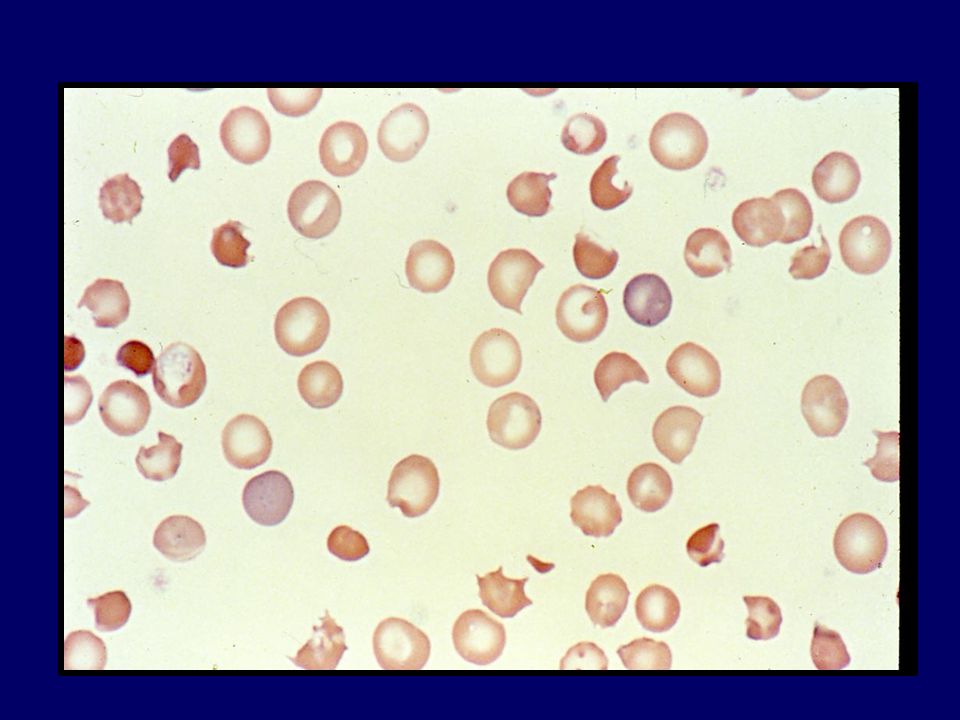
78
SICLE CELL ANEMIA Substitution glutamate valin on 6. position chain: Hb polymerisation, deformation of erythrocyte, tvaru sickle cell. hemolýza extravscular + intravascular (small vessel obstruction) Autosomal dominant type homozygotic form – both chains impaired heterozygotic form – one chain impaired 25-50% HbS – sickle cell trait
 Autosomal dominant type. homozygotic form – both chains impaired. heterozygotic form – one chain impaired % HbS – sickle cell trait.")
79
SRPKOVITÁ ANÉMIE Clinicaly: Hemolytic + aplastic crisis, splenomegaly, Diagnostics krevní obraz – anemie s retikulocytozou a srpkovitými ery elfo hemoglobinu – přítomnost Hb S identifikace Hb S peptickým štěpením globinu molekul.genetika – analýza DNA - v prenatální péči Treatment: Crisis prevention, transfusions, SCT

80
NEIMUNNÍ ZÍSKANÉ HEMOLYTICKÉ ANÉMIE
MECHANICKÉ A FYZIKÁLNÍ PŘÍČINY vadná srdeční chlopeň pochodová hemoglobinurie mikroangiopatické hemolytické anémie rozsáhlé popáleniny METABOLICKÉ PŘÍČINY jaterní choroby, alkoholismus hypofosfatémie hereditární abetalipoproteinemie podvýživa nadbytek mědi, Wilsonova choroba CHEMICKÉ LÁTKY oxidační činidla, hadí jedy INFEKCE přímá infekce erytrocytů: malárie aj. septikémie ( clostridium perfringens aj. ) leptospiry, borelie.
 leptospiry, borelie.")
81
MIKROANGIOPATICKÁ HEMOLYTICKÁ ANÉMIE
příčina: rozrušení integrity membrány erytrocytu mechanickou příčinou v průsvitu cévy, nejčastěji depozity fibrinu v místě poškození endotelu cévní stěny. Vaskulitidy, akutní glomerulonefritis, po SCT, nádory, operace chlopní, AV malformace, léky – ticlopidin, infekce – Shigatoxin. fragmentace krvinek – schistocyty – zvýšený zánik ve slezině, při masivní hemolýze – intravaskulární hemolýza při současné aktivaci kaogulačního systému – DIC s tvorbou mikrotrombů v cirkulaci. klinický obraz : dán kombinací hemolytické anémie, trombocytopénie a přítomnosti mikrotrombů (CNS, ledviny ) HUS, TTP, HELLP v graviditě – hemolýza, poruchy jaterních funkcí, trombocytopenie, DIC.
 HUS, TTP, HELLP v graviditě – hemolýza, poruchy jaterních funkcí, trombocytopenie, DIC.")
82
Patofyziologie HUS a diagnostika
toxin aktivace endotelu aktivace monocytů zánik endotelií sekrece cytokinů sekrece vWF exprese adhezivních molekul sekrece cytokinů deskvamace endotelií aktivace trombocytů adheze a invaze neutrofilů adheze trombocytů trombocytopenie okluze glomerulů MAHA renální selhání aktivace neutrofilů poškození endotelií elastázy, proteázy, H2O2

83
MIKROANGIOPATICKÁ HEMOLYTICKÁ ANÉMIE
Laboratorní nález: anémie s retikulocytózou, schistocyty, akantocyty, sférocyty, trombocytopenie se známkami DIC, nález multimerů při elfo vWF při TTP, molekulárně genetické vyšetření. Zvýšen přímý i nepřímý bilirubin v séru, zvýšení LDH, proteinurie, Hburie, zvýšen volný Hb, kreatinin, urea. Léčba: léčba vyvolávající příčiny, u TTP/HUS plasmaferéza se substitucí čerstvou zmrazenou plasmou, kortikoidy, antikoagulancia, transfuze erytrocytů.

85
AUTOIMMUNE HEMOLYTIC ANAEMIA Clasification
HEAT antibodies - idiopatic - secondary (lymfoproliferation, other type of tumours, autoimmune diseases, viral infections, immunodefficiency) -drug induced HA COLD antibodies - secondary (lymfoproliferation, viral inf., mykoplasma, autoimmune diseases - paroxysmal cold haemoglobinuria (lues …) MIXED HEAT AND COLD antibodies
 -drug induced HA. COLD antibodies. - secondary (lymfoproliferation, viral inf., mykoplasma, autoimmune diseases. - paroxysmal cold haemoglobinuria (lues …) MIXED HEAT AND COLD antibodies.")
86
Pathogenesis of AIHA: Cooperation disorder among supresor T helper T lymphocytes and B lymphocytes responsible for immunity control Dysregulation of this system leads to insufficient supression of antibody formation against own antigens

87
IgG – monomér, Fc část – vazebné místo pro C1q složku komplementu a Fcγ receptor makrofágů.
IgM – pentamér, Fc část – vazebné místo pro C1q složku komplementu a Fcγ receptor makrofágů.

88
HEAT ANTIBODIES IgG character – optimal at 370C
Catch up of erythrocytes with binded antibody by spleen macrophages EXTRAVASCULAR HEMOLYSIS Activation of complement by high antibody titre INTRAVACULAR HEMOLYSIS

89
COLD ANTIBODIES IgM character – optimál at 40C
Bound to erytrocytes in colder acral parts, possibility of complement activation, ery aglutination INTRAVASCULAR HEMOLYSIS EXTRAVASCULAR HEMOLYSIS

90
Secondary AIHA with heat antibodies
AUTOIMMUNE DISEASES systemic lupus erytematodes, revmatoid arthritis, sclerodermia, ulcerose colitis, syndrome of antiphospholipid antibodies HEMATOLOGIC TUMOURS chronic lymphadenosis,malign lymphomas, rarely acute leucaemia OTHER TUMOURS carcinoma, thymoma, Kaposi sarkoma, teratoma INFECTIONS EBV, HIV-1,2, HCV, vaccination (difteria-pertusis-tetanus) IMUNODEFICIENCY congenital and acquired hypogamaglobulinemia and dysgamaglobulinemia
 IMUNODEFICIENCY. congenital and acquired hypogamaglobulinemia and. dysgamaglobulinemia.")
91
DRUG-INDUCED HEMOLYTIC ANAEMIA
hapten type imunocomplex type De-novo antigen formation

92
AIHA –laboratory parameters:
Blood count: makrocytic anaemia with reticulocytosis Biochemistry: direct and indirect bilirubin, urobilinogen in urine Special tests: Direct and indirect antiglobuline test (Coombs test) INTRAVASCULAR HEMOLYSIS PROOF: free Hb in plasma, levels of haptoglobin and hemopexin in serum, hemoglobinuria
 INTRAVASCULAR HEMOLYSIS PROOF: free Hb in plasma, levels of haptoglobin and hemopexin in serum, hemoglobinuria.")
93
DIRECT COOMBS TEST Erytrocytes with bound Ab We add : anti IgG

94
INDIRECT COOMBS TEST Sérum with free antibodies
we add: erythrocytes of particular blood group we add : anti IgG or anti C3b

95
AIHA – diferential diagnosis:
CORPUSCULAR HEMOLYTIC ANAEMIA negative Coombs test, positive special tests (autohemolysis, erytrocyte enzyme tests, elfo Hb, shortened lifespan of autologous, not donor erythrocytes) PAROXYSMÁL NIGHT HAEMOGLOBINURIA negative Coombs test, pancytopenia, CD59 and CD55 antigen defficiency on erythrocytes, CD14 antigen def. on the surface of granulocytes and monocytes GILBERT DISEASE- negative hemolysis tests NON- IMMUNE HEMOLYTIC ANAEMA microangiopatic hemolytic anemia (schistocytes, kidney and CNS affection), anemia from physical and chemical causes MYELODYSPLASTIC SYNDROME - hemolytic form morfological dysplastic changes,chromosomal aberances,cytochemical changes, clonality.
 PAROXYSMÁL NIGHT HAEMOGLOBINURIA. negative Coombs test, pancytopenia, CD59 and CD55 antigen defficiency on erythrocytes, CD14 antigen def. on the surface of granulocytes and monocytes. GILBERT DISEASE- negative hemolysis tests. NON- IMMUNE HEMOLYTIC ANAEMA. microangiopatic hemolytic anemia (schistocytes, kidney and CNS affection), anemia from physical and chemical causes. MYELODYSPLASTIC SYNDROME - hemolytic form. morfological dysplastic changes,chromosomal aberances,cytochemical changes, clonality.")
96
AIHA - treatment: Light form ( Hb > 80 g/l ):
PREDNISONE 1 mg/kg/d 2-3 weeks - in case of good effect decreasing dose every 2-3 days by 10mg until 20 mg/day. - slow reduction of dose (by 5mg in 7-10 days) until 5-10mg every second day. - end of corticooid therapy when repeated direct Coombs test negativity When therapy is ineffective or relaps occurs: combination with CYCLOPHOSPHAMIDE mg/d or CYCLOSPORINE A 3 mg/kg/d.
 until 5-10mg every second day. - end of corticooid therapy when repeated direct Coombs test negativity. When therapy is ineffective or relaps occurs: combination with. CYCLOPHOSPHAMIDE mg/d or. CYCLOSPORINE A 3 mg/kg/d.")
97
AIHA - treatment: SEVERE form ( Hb < 80 g/l ):
PREDNISONE 1-2 g i.v. daily 5 days, after that in case of good response fast decrese of dose to 1 mg/kg. - combination of corticoids with : CYCLOPHOSPHAMIDE 200 mg i.v./d i.v. IMMUNOGLOBULINS 0,5g /kg/d PLASMAPHERESIS RITUXIMAB (anti CD20 monoclonal Ab) Transfusion – together with corticoids , monitored hospitalised patient, not more then 1 TU/day (unless vital indication)
 Transfusion – together with corticoids , monitored hospitalised patient, not more then 1 TU/day (unless vital indication)")
98
Thank you

Podobné prezentace






 all morning! John isn´t here. He _______ (go) to the.>")
















