Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Patofyziologie ledvin
EVROPSKÝ SOCIÁLNÍ FOND Patofyziologie ledvin MUDr. Klára Bernášková, CSc. Ústav normální, patologické a klinické fyziologie PRAHA & EU INVESTUJEME DO VAŠÍ BUDOUCNOSTI

2
Funkce ledvin Homeostatické Endokrinní Metabolické
Metabolismus vody a iontů Udržování krevního tlaku Vylučování zplodin metabolismu, toxických látek a léků Udržování acidobazické rovnováhy Endokrinní (Renin) Erytropoetin, Trombopoetin Kalcitriol Degradace PTH a inzulinu Metabolické Glukoneogeneze
 Erytropoetin, Trombopoetin. Kalcitriol. Degradace PTH a inzulinu. Metabolické. Glukoneogeneze.")
3
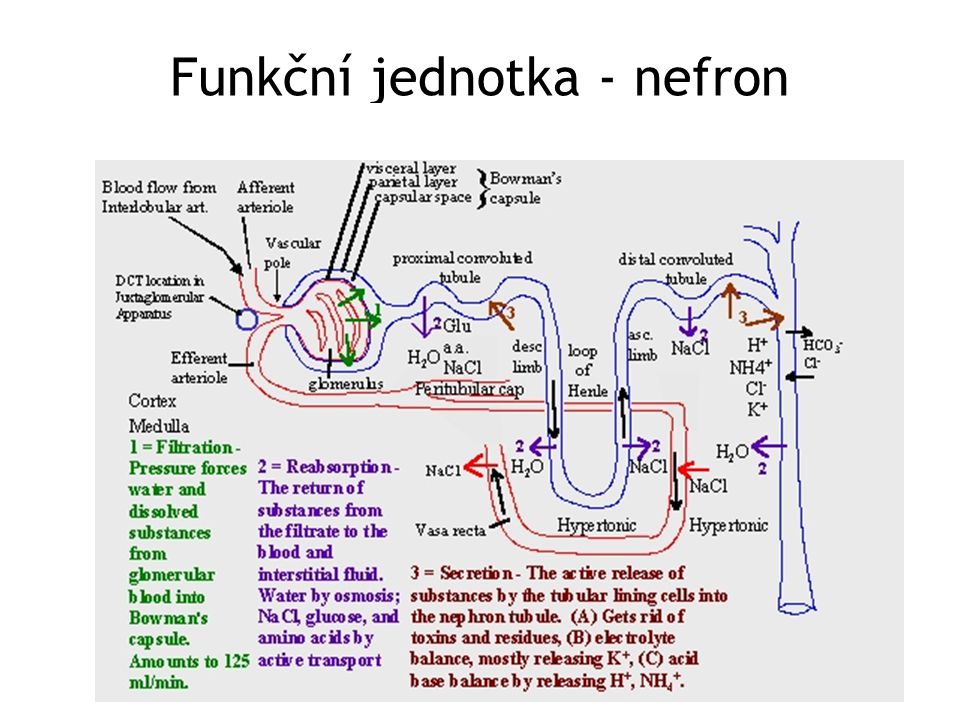
Funkční jednotka - nefron
4
Řízení funkce ledvin Autroregulace průtoku krve ledvinami ( torr) - myogenní reflex (Baylissův reflex) - angiotenzin II - prostaglandiny z mesangia - tubuloglomerulární zpětná vazba Resorpce z proximálního tubulu - sympatikus - ANP Resorpce z distálního tubulu - aldosteron - ADH - PTH

5
Poruchy funkce glomerulu
Nefritický syndrom Vzniká jako důsledek zánětu - (edém, celularizace, lokální defekty membrány) Proteinurie, hematurie, hypertenze (edém) Hereditární glomerulonefritida: Alportův sy Získaná: akutní, chronická Nefrotický syndrom Nephritic syndrome is a manifestation of glomerular inflammation (glomerulonephritis [GN]) and occurs at any age. Causes differ by age and mechanisms differ by cause. The syndrome can be acute or chronic and primary (idiopathic) or secondary. Is defined by hematuria and the presence of dysmorphic RBCs and RBC casts on microscopic examination of urinary sediment. Often ≥ 1 of the following elements are present: mild to moderate proteinuria, hypertension, edema, elevated serum creatinine, and oliguria. Diagnosis is based on history, physical examination, and sometimes renal biopsy. Treatment and prognosis vary by cause. Hereditary Nephritis (Alport's Syndrome) Hereditary nephritis is a genetically heterogenous disorder characterized by hematuria, impaired renal function, sensorineural deafness, and ocular abnormalities. Cause is a gene mutation affecting type IV collagen. Symptoms and signs are those of nephritic syndrome (ie, hematuria, eventual renal insufficiency) often with sensorineural deafness and, less commonly, ophthalmologic symptoms. Nephrotic syndrome is kidney disease with proteinuria, hypoalbuminemia, hyperhcolesterolemia, thrombofilia and edema. Nephrotic-range proteinuria is 3, 5 grams per day or more. There are many specific causes of nephrotic syndrome. These include kidney diseases such as minimal-change nephropathy, focal glomerulosclerosis, and membranous nephropathy. Nephrotic syndrome can also result from systemic diseases that affect other organs in addition to the kidneys, such as diabetes, amyloidosis, and lupus erythematosus. Nephrotic syndrome may affect adults and children, of both sexes and of any race. It may occur in typical form, or in association with nephritic syndrome. The latter connotes glomerular inflammation, with hematuria and impaired kidney function. Nephrotic-range proteinuria may occur in other kidney diseases, such as IgA nephropathy. In that common glomerular disease, one third of patients may have nephrotic-range proteinuria.[1] Nephrotic syndrome may occur in persons with sickle cell disease and evolve to renal failure. Membranous nephropathy may complicate bone marrow transplantation, in association with graft versus host disease. Kidney diseases that affect tubules and interstitium, such as interstitial nephritis, will not cause nephrotic syndrome.
 Proteinurie, hematurie, hypertenze (edém) Hereditární glomerulonefritida: Alportův sy. Získaná: akutní, chronická. Nefrotický syndrom. Nephritic syndrome is a manifestation of glomerular inflammation (glomerulonephritis [GN]) and occurs at any age. Causes differ by age and mechanisms differ by cause. The syndrome can be acute or chronic and primary (idiopathic) or secondary. Is defined by hematuria and the presence of dysmorphic RBCs and RBC casts on microscopic examination of urinary sediment. Often ≥ 1 of the following elements are present: mild to moderate proteinuria, hypertension, edema, elevated serum creatinine, and oliguria. Diagnosis is based on history, physical examination, and sometimes renal biopsy. Treatment and prognosis vary by cause. Hereditary Nephritis. (Alport s Syndrome) Hereditary nephritis is a genetically heterogenous disorder characterized by hematuria, impaired renal function, sensorineural deafness, and ocular abnormalities. Cause is a gene mutation affecting type IV collagen. Symptoms and signs are those of nephritic syndrome (ie, hematuria, eventual renal insufficiency) often with sensorineural deafness and, less commonly, ophthalmologic symptoms. Nephrotic syndrome is kidney disease with proteinuria, hypoalbuminemia, hyperhcolesterolemia, thrombofilia and edema. Nephrotic-range proteinuria is 3, 5 grams per day or more. There are many specific causes of nephrotic syndrome. These include kidney diseases such as minimal-change nephropathy, focal glomerulosclerosis, and membranous nephropathy. Nephrotic syndrome can also result from systemic diseases that affect other organs in addition to the kidneys, such as diabetes, amyloidosis, and lupus erythematosus. Nephrotic syndrome may affect adults and children, of both sexes and of any race. It may occur in typical form, or in association with nephritic syndrome. The latter connotes glomerular inflammation, with hematuria and impaired kidney function. Nephrotic-range proteinuria may occur in other kidney diseases, such as IgA nephropathy. In that common glomerular disease, one third of patients may have nephrotic-range proteinuria.[1] Nephrotic syndrome may occur in persons with sickle cell disease and evolve to renal failure. Membranous nephropathy may complicate bone marrow transplantation, in association with graft versus host disease. Kidney diseases that affect tubules and interstitium, such as interstitial nephritis, will not cause nephrotic syndrome.")
6
Nefrotický syndrom (proteinurie 3,5 g/den)
Poškození glomerulární membrány toxické poškozování tubulů Toxic injury to tubules transportních prot. proteinurie Proteinuria retence Na+ a vody (sympatikus, ADH, aldosteron) Ab, proteinů akutní f. antikoagulačních p. ztráty bílkovin cirkulující objem ↓ Circulating volume generalizované edémy Generalised edema onkotického tlaku hyperkoagulační stav Thrombogenesis produkce fibrinogenu metabolismus lipidů metabolismu v játrech Liver metabolism dyslipidemie Dyslipidaemia aterogenesis aterogeneze
 Ab, proteinů akutní f. antikoagulačních p. ztráty bílkovin. cirkulující objem. ↓ Circulating volume. generalizované edémy. Generalised edema. onkotického tlaku. hyperkoagulační stav. Thrombogenesis. produkce fibrinogenu. metabolismus lipidů. metabolismu v játrech. Liver metabolism. dyslipidemie. Dyslipidaemia. aterogenesis. aterogeneze.")
7
Tubulointersticiální onemocnění
Vrozené Renální diabetes insipidus Renální diabetes mellitus Fosfátový diabetes Aminoacidurie RTA Fanconiho syndrom Polycystické ledviny Phosphate diabetes, tubular phosphate reabsorption and phosphatonins. Laroche M, Boyer JF. Phosphate diabetes is defined as inadequate tubular reabsorption. Hypophosphatemia is responsible for most of the clinical manifestations, which vary with the age of the patient and the severity of the phosphate wasting. Vitamin D-resistant rickets in children or osteomalacia in adults, osteoporosis, bone pain including spinal pain, and pain in the joints and periarticular areas are the main manifestations. Several factors are known to affect tubular phosphate reabsorption via the sodium/phosphate cotransporters located on the tubular cell membranes. Factors that decrease phosphate reabsorption include a high intake of dietary phosphate, acidosis, parathyroid hormone (PTH), PTH-related peptide (PTHrp), glucocorticoid therapy, calcitonin, and vitamin D. On the other hand, a low-phosphate diet, alkalosis, growth hormone, insulin, IGF-1, and thyroid hormones increase tubular phosphate reabsorption. Physiological concepts about tubular phosphate reabsorption have been radically changed by the recent identification of phosphaturic factors called phosphatonins. The most extensively studied phosphatonin to date is fibroblast growth factor 23 (FGF23), which was first identified in patients with tumor-induced osteomalacia and shown to be secreted by the neoplastic cells. The FGF23 has also been implicated in autosomal dominant hypophosphatemic rickets, in which a gene mutation results in production of abnormal FGF23 that resists hydrolysis. In healthy individuals, FGF23 contributes to regulate phosphate reabsorption via Na/Pi cotransporters. Other phosphatonins may exist, such as matrix extracellular phosphoglycoprotein (MEPE) and secreted frizzled-related protein 4 (SFRP4), whose role remains to be defined. The part played by these proteins in idiopathic renal phosphate wasting in adults needs to be investigated. Cystinuria is characterized by the inadequate reabsorption of cystine in the proximal convoluted tubules after the filtering of the amino acids by the kidney's glomeruli, thus resulting in an excessive concentration of this amino acid in the urine. Cystine may precipitate out of the urine, if the urine is neutral or acidic, and form crystals or stones in the kidneys, ureters, or bladder. It is one of several inborn errors of metabolism included in the Garrod's tetrad. The disease is attributed to deficiency in transport and metabolism of amino acids. Cystinuria is a cause of persistent kidney stones. It is a disease involving the defective transepithelial transport of cystine and dibasic amino acids in the kidney and intestine, and is one of many causes of kidney stones. If not treated properly, the disease could cause serious damage to the kidneys and surrounding organs, and in some rare cases death. Chemical structure of cystine formed from L-cysteine (under biological conditions) Hartnup‘s disease Hartnup disease is an autosomal recessive disorder caused by impaired neutral (ie, monoaminomonocarboxylic) amino acid transport in the apical brush border membrane of the small intestine and the proximal tubule of the kidney. Patients present with pellagralike skin eruptions, cerebellar ataxia, and gross aminoaciduria. Fanconi‘s syndrome: Fanconi's syndrome is a set of kidney malfunctions brought about by a variety of seemingly unrelated disorders. Kidney malfunction leads to excessive urine production and excessive thirst, resulting in deficits of water, calcium, potassium, magnesium, and other substances in the body. It often leads to bone disease and stunted growth. Description: Proximal tubule reabsorption is defective in Fanconi's syndrome. As a consequence, substances that are normally reabsorbed, like glucose, amino acids, small proteins, water, calcium, potassium, magnesium, bicarbonate, and phosphate, are lost and the body becomes overly acidic. Causes: Fanconi's syndrome can be caused by a variety of genetic defects and by certain environmental assaults.The genetic diseases known to give rise to Fanconi's syndrome are cystinosis (the most common cause in children), galactosemia, glycogen storage disease, hereditary fructose intolerance, Lowe syndrome, Wilson disease, tyrosinemia, medullary cystic disease, vitamin D dependency, and familial idiopathic Fanconi's syndrome. Environmental assaults that cause Fanconi's syndrome include exposure to heavy metals (like cadmium, lead, mercury, platinum, uranium), certain drugs (like outdated tetracycline and gentamicin), other substances (like Lysol, paraquat, toluene, the amino acid lysine taken as a nutritional supplement), and kidney transplantation.
, PTH-related peptide (PTHrp), glucocorticoid therapy, calcitonin, and vitamin D. On the other hand, a low-phosphate diet, alkalosis, growth hormone, insulin, IGF-1, and thyroid hormones increase tubular phosphate reabsorption. Physiological concepts about tubular phosphate reabsorption have been radically changed by the recent identification of phosphaturic factors called phosphatonins. The most extensively studied phosphatonin to date is fibroblast growth factor 23 (FGF23), which was first identified in patients with tumor-induced osteomalacia and shown to be secreted by the neoplastic cells. The FGF23 has also been implicated in autosomal dominant hypophosphatemic rickets, in which a gene mutation results in production of abnormal FGF23 that resists hydrolysis. In healthy individuals, FGF23 contributes to regulate phosphate reabsorption via Na/Pi cotransporters. Other phosphatonins may exist, such as matrix extracellular phosphoglycoprotein (MEPE) and secreted frizzled-related protein 4 (SFRP4), whose role remains to be defined. The part played by these proteins in idiopathic renal phosphate wasting in adults needs to be investigated. Cystinuria is characterized by the inadequate reabsorption of cystine in the proximal convoluted tubules after the filtering of the amino acids by the kidney s glomeruli, thus resulting in an excessive concentration of this amino acid in the urine. Cystine may precipitate out of the urine, if the urine is neutral or acidic, and form crystals or stones in the kidneys, ureters, or bladder. It is one of several inborn errors of metabolism included in the Garrod s tetrad. The disease is attributed to deficiency in transport and metabolism of amino acids. Cystinuria is a cause of persistent kidney stones. It is a disease involving the defective transepithelial transport of cystine and dibasic amino acids in the kidney and intestine, and is one of many causes of kidney stones. If not treated properly, the disease could cause serious damage to the kidneys and surrounding organs, and in some rare cases death. Chemical structure of cystine formed from L-cysteine (under biological conditions) Hartnup‘s disease Hartnup disease is an autosomal recessive disorder caused by impaired neutral (ie, monoaminomonocarboxylic) amino acid transport in the apical brush border membrane of the small intestine and the proximal tubule of the kidney. Patients present with pellagralike skin eruptions, cerebellar ataxia, and gross aminoaciduria. Fanconi‘s syndrome: Fanconi s syndrome is a set of kidney malfunctions brought about by a variety of seemingly unrelated disorders. Kidney malfunction leads to excessive urine production and excessive thirst, resulting in deficits of water, calcium, potassium, magnesium, and other substances in the body. It often leads to bone disease and stunted growth. Description: Proximal tubule reabsorption is defective in Fanconi s syndrome. As a consequence, substances that are normally reabsorbed, like glucose, amino acids, small proteins, water, calcium, potassium, magnesium, bicarbonate, and phosphate, are lost and the body becomes overly acidic. Causes: Fanconi s syndrome can be caused by a variety of genetic defects and by certain environmental assaults.The genetic diseases known to give rise to Fanconi s syndrome are cystinosis (the most common cause in children), galactosemia, glycogen storage disease, hereditary fructose intolerance, Lowe syndrome, Wilson disease, tyrosinemia, medullary cystic disease, vitamin D dependency, and familial idiopathic Fanconi s syndrome. Environmental assaults that cause Fanconi s syndrome include exposure to heavy metals (like cadmium, lead, mercury, platinum, uranium), certain drugs (like outdated tetracycline and gentamicin), other substances (like Lysol, paraquat, toluene, the amino acid lysine taken as a nutritional supplement), and kidney transplantation.")
8
Tubulointersticiální onemocnění
Získané Akutní tubulární poškození (Fanconiho sy) Akutní tubulární ischemie Renální diabetes insipidus Chronické tubulointersticiální onemocnění (poruchy) (aktivace buněk tubulů)
 Akutní tubulární ischemie. Renální diabetes insipidus. Chronické tubulointersticiální onemocnění (poruchy) (aktivace buněk tubulů)")
9
Důsledky poruchy homeostatických funkcí ledvin:
(Před ledvinami) Δ TK, edém hyperkalémie, hyperfosfatémie (hypokalcémie) azotémie, urémie, kreatininémie; urikémie metabolická acidóza V moči Δ specifické hmotnosti moči a objemu Δ iontů, pH - patologická příměs: proteiny, cukr, krev, hnis, krystaly, válce
 Δ TK, edém. hyperkalémie, hyperfosfatémie (hypokalcémie) azotémie, urémie, kreatininémie; urikémie. metabolická acidóza. V moči. Δ specifické hmotnosti moči a objemu. Δ iontů, pH. - patologická příměs: proteiny, cukr, krev, hnis, krystaly, válce.")
10
Selhání ledvin

11
Akutní renální selhání
„náhlá ztráta schopnosti ledvin odstraňovat z těla odpadní produkty a koncentrovat moč bez ztrát iontů“ Typy: prerenální intrarenální postrenální Kompenzatorní změna funkce = prerenální azotémie Selhání ledvin způsobené poškozením funkce tubulů

12
Akutní renální selhání - diferenciální diagnóza
Prerenální Intrarenální Postrenální Mechanismus Anamnéza ↓ cirkulující objem, akutní selhání srdce, ACEI/NSAID ischemie ledvin nefrotoxiny vaskulitidy ledvinné kameny nádor, hyperplazie prostaty Fyzikální vyšetření Hypotenze Hypovolémie, euvolémie nebo hypervolémie Naplněný močový měchýř, hyperplazie prostaty Poměr urea : kreatinin v séru Větší retence urey než kreatininu Retence urey i kreatininu stejná Zvýšená retence urey vlivem ADH ve fungujících tubulech Na+ v moči 20 mmol/l 40 mmo/l Aldosteron snižuje vylučování sodíku ledvinami (jen ve funkčních tubulech) Kreatinin v moči : kreatinin v séru 40 : 1 20 : 1 Retence vody vlivem ADH (jen ve funkčních tubulech), vysoká koncentrace moči Osmolarita moči : osmolarita plazmy 1,5 : 1 1,3 : 1 Koncentrační schopnost ledvin je zachovaná při funkčních tubulech Frakční exkrece sodíku 1% 1 -2 % Retence sodíku vlivem aldosteronu v nepoškozených tubulech
 Kreatinin v moči. : kreatinin v séru. 40 : : 1. Retence vody vlivem ADH (jen ve funkčních tubulech), vysoká koncentrace moči. Osmolarita moči : osmolarita plazmy. 1,5 : 1. 1,3 : 1. Koncentrační schopnost ledvin je zachovaná při funkčních tubulech. Frakční exkrece sodíku. 1% 1 -2 % Retence sodíku vlivem aldosteronu v nepoškozených tubulech.")
13
Stádia akutního renálního selhání
Oligouricko-anurické Snížený výdej vody, nadbytek zplodin metabolismu, porucha metabolismu iontů ↑ TK, otoky, ↑ urea, hyperkalémie, metabolická acidóza Polyurické ztráty velkého množství nekoncentrované moči, ztráty iontů Šok, srdeční selhání Stádium úzdravy (nebo přechod do chronického renálního selhávání) Urémie (uremický syndrom): ↑ urea, kreatinin, kyselina močová, ↑ K+, acidóza GIT: nauzea, zvracení, anorexie, krvavý průjem hemoragická diatéza: zvýšená krvácivost (destičky) příznaky z poruch CNS a PNS kardiovaskulární příznaky Uremia - clinical syndrome associated with fluid, electrolyte, and hormone imbalances and metabolic abnormalities, which develop in parallel with deterioration of renal function. Uremia more commonly develops with chronic renal failure (CRF) or the later stages of chronic kidney disease (CKD), but it also may occur with acute renal failure (ARF) if loss of renal function is rapid. As yet, no single uremic toxin has been identified that accounts for all of the clinical manifestations of uremia. Severe complications: seizure, coma, cardiac arrest, and death. Spontaneous bleeding (gastrointestinal (GI) bleeding, spontaneous subdural hematomas, increased bleeding from any underlying disorder, or bleeding associated with trauma).
 Urémie (uremický syndrom): ↑ urea, kreatinin, kyselina močová, ↑ K+, acidóza. GIT: nauzea, zvracení, anorexie, krvavý průjem. hemoragická diatéza: zvýšená krvácivost (destičky) příznaky z poruch CNS a PNS. kardiovaskulární příznaky. Uremia - clinical syndrome associated with fluid, electrolyte, and hormone imbalances and metabolic abnormalities, which develop in parallel with deterioration of renal function. Uremia more commonly develops with chronic renal failure (CRF) or the later stages of chronic kidney disease (CKD), but it also may occur with acute renal failure (ARF) if loss of renal function is rapid. As yet, no single uremic toxin has been identified that accounts for all of the clinical manifestations of uremia. Severe complications: seizure, coma, cardiac arrest, and death. Spontaneous bleeding (gastrointestinal (GI) bleeding, spontaneous subdural hematomas, increased bleeding from any underlying disorder, or bleeding associated with trauma).")
14
Chronické renální selhání (CRF)
„pomalá ztráta funkcí ledvin způsobená chronickým úbytkem nefronů“ Příčiny: všechna chronická onemocnění poškozující ledviny (hypertenze, diabetes, infekce ledvin, vaskulitidy, tubulointersticiální onemocnění, glomerulonefritidy, polycystické ledviny, amyloidóza)
")
15
Stádia chronického ledvinného selhávání
Stádium poškození GF 25 – 50 ml/min Polyurie, nykturie, izostenurie Stádium selhávání GF 20 ml/min Anémie, osteopatie, azotémie x dieta homeostázu udržuje Stádium selhání (End Stage Renal Disease (ESRD)) GF pod 10 ml/min Uremický syndrom, anémie, osteopatie ..hyperkalémie, acidóza..
) GF pod 10 ml/min. Uremický syndrom, anémie, osteopatie ..hyperkalémie, acidóza..")
16
Chronické renální selhání - důsledky
Poškození nebo ztráta nefronů glomerulární filtrace Porucha exkrečních funkcí: retence: perfuze ledvin Porucha renálních funkcí oligurie, anurie sodík a voda hypertenze edémy Porucha endokrinních funkcí: hyperkalémie K+ sekrece EPO Severe hypoglycemic reactions - in patients with diabetes if hyperglycemic medications are not adjusted for decreased creatinine clearance in these individuals. Renal failure associated bone disease (renal osteodystrophy) may lead to an increased risk of osteoporosis or bone fracture with trauma. anémie uremický syndrom urea sekrece inzulinázy ( gluconeogeneze) kyselina močová dna por. metabolizmu cukrů metabol. acidóza H+ odbourávání PTH renální osteopatie sekrece PTH fosfáty aktivace kalcitriolu
 may lead to an increased risk of osteoporosis or bone fracture with trauma. anémie. uremický syndrom. urea. sekrece inzulinázy. ( gluconeogeneze) kyselina močová. dna. por. metabolizmu cukrů. metabol. acidóza. H+ odbourávání PTH. renální osteopatie. sekrece. PTH. fosfáty. aktivace kalcitriolu.")
17
Příčiny renální anémie
snížená sekrece EPO chronické ztráty krve nedostatek železa nedostatek proteinů nedostatek vit. B12 nebo folátu chronické infekce nebo záněty snížená citlivost EPO receptorů poškození kostní dřeně toxicita hliníku nádory Přímý důsledek selhávání ledvin Malabsorpce, dieta Účinek ↑ PTH Jiné příčiny

18
Renální anémie Hemoglobin 110 -120 g/l Normochromní, normocytární
Srdeční selhání Selhání ledvin Anémie 18

19
Rozvoj renální osteopatie
Snížení počtu nefronů biosyntetické aktivity ledvin tvorby kalcitriolu resorpce vápníku v GIT exkrečních funkcí ledvin Retence toxických látek Metabolická acidóza Hyperfosfatémie Hypokalcémie sekrece PTH Osteitis fibrosa cystica Remodelace a redistribuce kosti =Osteoskleróza Metastatické kalcifikace Porucha poměru kalcium x fosfáty Kost jako „pufr“ Dekalcifikace +porucha matrix =Osteoporóza Proteino- -kalorická malnutrice Porucha růstu kostí u dětí (renální křevice) citlivost kosti na kalcitriol Osteomalácie Toxicita hliníku, warfarin
 citlivost kosti na kalcitriol. Osteomalácie. Toxicita hliníku, warfarin.")
20
Děkuji za pozornost

Podobné prezentace
















>")


