Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
DIAGNOSTIKA PORUCH HEMOKOAGULAČNÍ ROVNOVÁHY
Jan Živný Department of Pathophysiology

2
HEMOKOAGULAČNÍ ROVNOVÁHA
KREVNÍ DESTIČKY PLAZMATICKÝ KOAGULAČNÍ SYSTÉM KOAGULAČNÍ, FIBRINOLYTICKÝ, KALIKREIN-KININOVÝ CÉVNÍ STĚNA ENDOTEL Toto je na úvod - základní systémy jejichž kooperací je udržována hemokoagulační rovnováha. HEMOSTÁZA JE INTEGRÁLNÍ SOUČÁSTÍ ZÁNĚTOVÉ ODPOVĚDI

3
PORUCHY HEMOKOAGULAČNÍ ROVNOVÁHY - TROMBÓZA A EMBOLIE
V MIKROCIRKULACI ŽILNÍ ARTERIÁLNÍ K symptomatologii poruch hemokoagulační rovnováhy je nutné zdůraznit, že řada poruch má trombo-hemoragické projevy i v jedné fázi onemocnění. Je to především DIC, ale o DIC bude seminář na podzim, a proto ji probírat nebudu. Patří sem ale přítomnost antifosfolipidových protilátek například při SLE. Antifosfolipidové protilátky se projevují jako lupus antikoagulans a na druhé straně inhibují protein C systém a působí tak protromboticky. OBECNÉ PŘÍZNAKY - ISCHEMIE TKÁNÍ - OBĚHOVÉ SELHÁNÍ PLICNÍ SYSTÉMOVÁ EMBOLIE

4
Pathogenesis - Virchow postulated that thrombi formed as a result of the one or more abnormalities in: the blood bessel; the flow of the blood; and the coagulability of the blood.

5
Abnormal Blood Vessel Trauma Vasculitis Atherosclerosis Others

6
Abnormal Blood Flow Decreased mobility Vessel Obstruction
Eccomomy class syndrome Pregnancy

7
Abnormal Blood Abnormal Blood - hypercoagulable states a. Acquired
(1) Stress (a) Postoperative State (b) Pregnancy (c) Oral contraceptives (2) Lupus-Type Anticoagulant and the antiphospholipid syndrome - Autoantibodies that recognize phospholipid and protein prolong coagulation tests like the aPTT, but, paradoxically, through a variety of mechanisms, may lead to thrombosis. (3) Reduced natural anticoagulants (a) DIC - Leads to the consumption of both procoagulants and anticoagulants. (b) Malignancy (c) Nephrotic syndrome - Antithrombin and some contact factors are lost inthe urine in the nephrotic syndrome. (4) Abnormal Platelet Function (a) Myeloproliferative disorders - Malignant disorders of the bone marrow that lead to the production of abnormal platelets which may hyperfunction (leading the thrombosis) or hypofunction (leading to hemorrhage). (b) HIT (Heparin Induced Thrombocytopenia with thrombosis) (5) Abnormal Fibrinolysis - Plasminogen Deficiency, Contact Factor Deficiency
 Stress. (a) Postoperative State (b) Pregnancy (c) Oral contraceptives. (2) Lupus-Type Anticoagulant and the antiphospholipid syndrome - Autoantibodies that recognize phospholipid and protein prolong coagulation tests like the aPTT, but, paradoxically, through a variety of mechanisms, may lead to thrombosis. (3) Reduced natural anticoagulants. (a) DIC - Leads to the consumption of both procoagulants and anticoagulants. (b) Malignancy (c) Nephrotic syndrome - Antithrombin and some contact factors are lost inthe urine in the nephrotic syndrome. (4) Abnormal Platelet Function. (a) Myeloproliferative disorders - Malignant disorders of the bone marrow that lead to the production of abnormal platelets which may hyperfunction (leading the thrombosis) or hypofunction (leading to hemorrhage). (b) HIT (Heparin Induced Thrombocytopenia with thrombosis) (5) Abnormal Fibrinolysis - Plasminogen Deficiency, Contact Factor Deficiency.")
8
Abnormal Blood Inherited Deficiency or Abnormal Function of Natural Anticoagulants Abnormal FactorPrevalence*Factor VLeiden - APCR15-30%Prothrombin Gene Mutation7-10%Protein C5-6% Protein S5-6%Antithrombin III<1% *Prevalence is for first thrombosis #Remember that Factor VLeiden is a common mutation in northern Europeans, but has lower incidence in southern Europe and is essentially absent in the Asian and African-African populations.

9
Arterial Thrombi formed in higher flow
made up of primarily platelets and fibrin - white thrombus generally occlusive Arterial Thrombi: These thrombi are formed in higher flow,are made up of primarily platelets and fibrin (white thrombus), with layers enriched for fibrin and red blood cells called the lines of Zahn and are generally occlusive, leading to infarcition.
, with layers enriched for fibrin and red blood cells called the lines of Zahn and are generally occlusive, leading to infarcition.")
10
Venous Thrombi formed in lower flow
all of the celluar elements and fibrin – red thrombus tend to originate in the valve cusps Venous Thrombi: These thrombi are formed in lower flow, are made up of all of the celluar elements and fibrin (red thrombus). Formation is also generally cyclic, with layers enriched for fibrin and red blood cells (lines of Zahn). Thrombi in large veins tend to originate in the valve cusps.
. Formation is also generally cyclic, with layers enriched for fibrin and red blood cells (lines of Zahn). Thrombi in large veins tend to originate in the valve cusps.")
11
Venous Thrombi

12
Venous Thrombi

13
Fate of the Thrombus Resolution - complete healing Embolization
a. Resolution - complete healing b. Embolization - release from the site of formation and travel in the vessel to the next constriction. c. Organization - with recanalization or incorporation into the vessel wall Resolution - complete healing Embolization c. Organization - with recanalization or incorporation into the vessel wall

14
ŽILNÍ TROMBOEMBOLICKÁ NEMOC
INZULT min.- hod. DVT distální (infra)popliteální oblast DVT proximální iliofemorální oblast Příklad tromboembolické nemoci je uveden v klinické symptomatologii proto, že je epidemiologicky velmi závažná, a také proto, aby se zdůraznila možnost klinicky latentní fáze od inzultu k symptomu. roky hod. - dny Posttrombotický syndrom Plicní embolie
popliteální oblast. DVT proximální. iliofemorální oblast. Příklad tromboembolické nemoci je uveden v klinické symptomatologii proto, že je epidemiologicky velmi závažná, a také proto, aby se zdůraznila možnost klinicky latentní fáze od inzultu k symptomu. roky. hod. - dny. Posttrombotický syndrom. Plicní embolie.")
15
Prevalence of Congenital Thrombophilia
Factor General Population People With Thrombosis APCR: factor V Leiden mutation 3-8% of Caucasians 20-25% Prothrombin G20210A 2-3% of Caucasians 4-8% Antithrombin deficiency 1 in 1-1.8%% Protein C deficiency 1 in 300 % Protein S deficiency Unknown % Hyperhomocysteinemia 11% %

16
Relative Risk of First DVT or PE in Congenital Thrombophilia
Factor Odds of Thrombosis APCR: heterozygous factor V Leiden mutation 3x APCR: homozygous factor V Leiden mutation 18x Prothrombin G20210A heterozygotes 2-4.8x Antithrombin deficiency heterozygotes 10-20x Protein C deficiency heterozygotes 6.5x Protein S deficiency heterozygotes 1.6 to 11.5x

17
KLINICKÉ PŘÍZNAKY DVT/PE Časná hluboká žilní trombóza (DVT)
asymptomatická : způsobuje > 50% PE. B) symptomatická: otok pasivní bolest nebo palpační bolestivost, změny zbarvení a teploty kůže, Homansův příznak
 symptomatická: otok. pasivní bolest nebo palpační. bolestivost, změny zbarvení a teploty kůže, Homansův příznak.")
18
KLINICKÉ PŘÍZNAKY DVT/PE Posttrombotický syndrom
Příznaky chronické DVT - s latencí let po inzultu Následkem rozvoje DVT Náplň povrchových kolaterálních žil Lipodermatoskleróza, varixy, Ulcerace kůže DK - 50% v důsledku DVT.

19
KLINICKÉ PŘÍZNAKY DVT/PE Plicní embolie (PE)
Dle závažnosti: dyspnoe, tachypnoe, tachykardie pleuritická bolest na hrudi zvýšená náplň krčních žil hemoptýza oběhová nestabilita oběhové selhání až náhlá smrt

20
Klinická diagnostika DVT
Ultrazvuk s barevným Dopplerovým měřením Impedanční pletysmografie Magnetická rezonance (MRI) Kontrastní venografie Vychytávání I125Fibrinogenu ? Metody označené otazníkem jsou málo specifické i senzitivní pro danou diagnostiku. Metoda vychytávání I125 FBG je vysoce falešně pozitivní pro diagnostiku DVT.
 Kontrastní venografie. Vychytávání I125Fibrinogenu Metody označené otazníkem jsou málo specifické i senzitivní pro danou diagnostiku. Metoda vychytávání I125 FBG je vysoce falešně pozitivní pro diagnostiku DVT.")
21
Klinická diagnostika PE
Ventilačně perfúzní plicní scan Plicní angiografie CT Pravostranná srdeční katetrizace Echokardiografie Arteriální krevní plyny ? EKG ? RTG hrudníku ?

22
Laboratorní vyšetření hyperkoagulačních stavů
Anti-fosfolipidové prtilátky: Immunoassay (ELISA, RIA) APCR (Activated Protein C Resistence) Factor V Leiden a Prothrombin pomocí „Polymerase Chain Reaction“ (PCR) Měření specifických antikoagulačních proteinů Vyšetření fibrinolytického systému - aktivátorů plazminogenu tPA , uPA a jeho inhibitoru PAI-1, stanovení plazminogenu, jeho inhibitoru alfa2AP, stanovení lipoproteinu Lp (a) Persistence over time (repeat testing in >6 weeks)
 APCR (Activated Protein C Resistence) Factor V Leiden a Prothrombin pomocí „Polymerase Chain Reaction (PCR) Měření specifických antikoagulačních proteinů. Vyšetření fibrinolytického systému - aktivátorů plazminogenu tPA , uPA a jeho inhibitoru PAI-1, stanovení plazminogenu, jeho inhibitoru alfa2AP, stanovení lipoproteinu Lp (a) Persistence over time (repeat testing in >6 weeks)")
23
Laboratorní vyšetření hyperkoagulačních stavů
FDP - imunologické stanovení celkových degradačních produktů fibri(noge)nu (normál: < 1000 ug/L), ELISA nebo aglutinační semikvant. metody. Diagnostika hemokoagulačního rozvratu. Vysoké FDP při hyperfibrino(geno)lýze. D-dimer - imunologické stanovení FDP specifických pro stabilizovaný fibrin (normál < 500 ug/L). Zvýšení D-dimeru je vysoce senzitivní pro diagnostiku DVT/PE AT - funkční test stanovení aktivity antitrombinu v plazmě (normál % aktivity kontrolní plazmy) Při dysregulaci trombinu se AT spotřebovává v inhibičním komplexu TAT, kofaktorem je heparin. Primární nebo sekundární deficience AT (< 75%) představuje riziko trombofilie až rozvoje DIC.
nu (normál: < 1000 ug/L), ELISA nebo aglutinační semikvant. metody. Diagnostika hemokoagulačního rozvratu. Vysoké FDP při hyperfibrino(geno)lýze. D-dimer - imunologické stanovení FDP specifických pro stabilizovaný fibrin (normál < 500 ug/L). Zvýšení D-dimeru je vysoce senzitivní pro diagnostiku DVT/PE. AT - funkční test stanovení aktivity antitrombinu v plazmě (normál % aktivity kontrolní plazmy) Při dysregulaci trombinu se AT spotřebovává v inhibičním komplexu TAT, kofaktorem je heparin. Primární nebo sekundární deficience AT (< 75%) představuje riziko trombofilie až rozvoje DIC.")
24
D-DIMER Reference Range: nG/mL The specimen for the d-dimer can be either serum or an anticoagulated (citrate or EDTA) specimen. D-Dimer is a type of FDP that is derived only from plasmin action on fibrin. It is composed of the terminal D domains from two fibrinogen molecules that have been covalently linked by thrombin and factor XIII activity, then cleaved by plasmin. Microparticle agglutination (latex or polystyrene microparticles) are used to assay d-dimer. As with the macro latex agglutination, particles are coated with monoclonal antibody to D-Dimer. The difference is that the particle size is small enough the remain in a suspension, allowing turbidometric endpoint determination in automated instruments. The sensitivity and specificity are similar to that of the ELISA assays. Clinical Significance - When evaluating patients for suspected venous thromboembolism, the finding of a negative test can be helpful in excluding the condition if a sufficiently sensitive assay is being used to measure the D-Dimer. The FDP has not been demonstrated to be helpful in this regard. D-Dimer and FDP are elevated modestly whenever there is intravascular (venous or arterial) thrombosis such as myocardial infarction, stroke, peripheral vascular disease, deep venous thrombosis, or pulmonary embolism. D-Dimer and FDP are elevated modestly whenever there is an episode of hemostasis as in the post operative period or in association with trauma. D-Dimer and FDP are elevated (mild to marked) in disseminated intravascular coagulation (DIC), acute or chronic. D-Dimer and FDP are elevated (mild to marked) in pre-eclampsia. FDP, but not D-Dimer, will detect the degradation products of fibrinogen, therefore a discrepancy of elevated FDP without elevated D-Dimer would indicate accelerated lysis of fibrinogen as can be seen in DIC or, rarely, in primary fibrinogenolysis
 specimen. D-Dimer is a type of FDP that is derived only from plasmin action on fibrin. It is composed of the terminal D domains from two fibrinogen molecules that have been covalently linked by thrombin and factor XIII activity, then cleaved by plasmin. Microparticle agglutination (latex or polystyrene microparticles) are used to assay d-dimer. As with the macro latex agglutination, particles are coated with monoclonal antibody to D-Dimer. The difference is that the particle size is small enough the remain in a suspension, allowing turbidometric endpoint determination in automated instruments. The sensitivity and specificity are similar to that of the ELISA assays. Clinical Significance - When evaluating patients for suspected venous thromboembolism, the finding of a negative test can be helpful in excluding the condition if a sufficiently sensitive assay is being used to measure the D-Dimer. The FDP has not been demonstrated to be helpful in this regard. D-Dimer and FDP are elevated modestly whenever there is intravascular (venous or arterial) thrombosis such as myocardial infarction, stroke, peripheral vascular disease, deep venous thrombosis, or pulmonary embolism. D-Dimer and FDP are elevated modestly whenever there is an episode of hemostasis as in the post operative period or in association with trauma. D-Dimer and FDP are elevated (mild to marked) in disseminated intravascular coagulation (DIC), acute or chronic. D-Dimer and FDP are elevated (mild to marked) in pre-eclampsia. FDP, but not D-Dimer, will detect the degradation products of fibrinogen, therefore a discrepancy of elevated FDP without elevated D-Dimer would indicate accelerated lysis of fibrinogen as can be seen in DIC or, rarely, in primary fibrinogenolysis.")
25
PORUCHY HEMOKOAGULAČNÍ ROVNOVÁHY - KRVÁCENÍ
Z MALÝCH TRAUMAT - sc., im.vpichy - eroze na sliznicích DIFUZNÍ MIKROVASKULÁRNÍ - purpury - petechie, ekchymozy (>3 mm) - orgánové apoplexie CHIRURGICKÉ Rozlišení typu krvácení je pro klinickou diferenciální diagnostiku velmi zásadní. A) trombocytopenie B) desintegrace mikrovaskulární intimy nadhraniční trauma i při funkční hemostáze selhání posttraumatické hemostázy - dysfunkce D, PKS, E
 - orgánové apoplexie. CHIRURGICKÉ. Rozlišení typu krvácení je pro klinickou diferenciální diagnostiku velmi zásadní. A) trombocytopenie. B) desintegrace mikrovaskulární intimy. nadhraniční trauma i při funkční hemostáze. selhání posttraumatické hemostázy - dysfunkce D, PKS, E.")
26
KREVNÍ DESTIČKY Platelet blood components may be stored for 5 days at room temperature

27
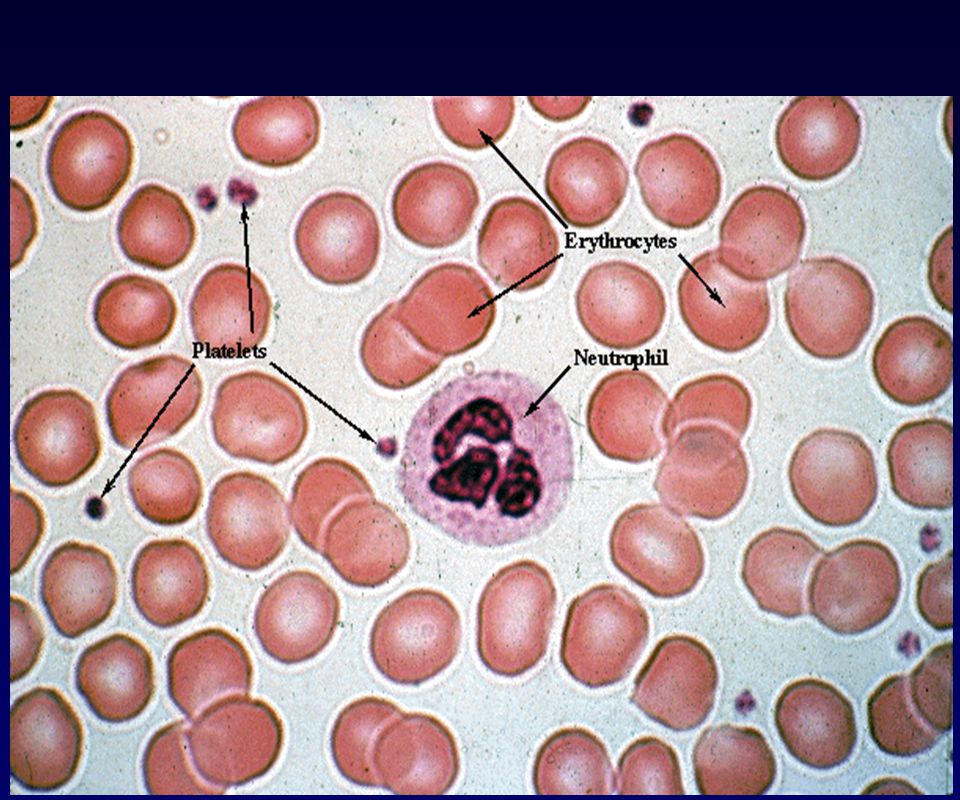
KREVNÍ DESTIČKY 150,000 to 350,000/µl. (below 50,000/µl = danger of uncontrolled bleeding). von Willebrand factor links exposed collagen to platelets forming a plug of platelets there. The bound platelets release ADP and thromboxane A2 recruiting more platelets circulating in the blood.

29
Idiopathic Thrombocytopenic Purpura
Large ecchymotic area over the thigh following minor trauma. The platelet count at the time was 7000/uL Bone marrow biopsy showing both megakaryocytic and erythroid hyperplasia

30
Destičky a von Willebrand factor
Počet destiček (PLT) - 150k - 400k /mL pro chirurgický zákrok optimální > 100k /mL těžká trombocytopenie < 20k /mL (spontální krvácení) Mean platelet volume (MPV) fL Aggregometrie Klasifikace kongenitálních trombocytopatií Agregace je indukovaná v PRP nebo v PB odebrané do citrátu sodného (ACD) přidáním aktivátoru (ADP, trombin, collagen) EDTA - induced PLT clumping - result in low PLT count - is an artifact which should be excluded by the peripheral blood smear evaluation and repetition of PLT count using a blood sample collected to sodium citrate RISTOCETIN IS ANTIBIOTICS WHICH INTERACTS WITH THE GP Ib ON THE PLT SURFACE AND WITH vWF IN PLASMA TO INDUCE CONFORMATION CHANGES WHICH ALLOW vWF TO BIND ON GP Ib WHICH LEADS TO AGGREGATION (MOST vWD EXCEPT TYPE 2B). some hereditary thrombocytopaties have large PLT PLT LABORATORY
 - 150k - 400k /mL. pro chirurgický zákrok optimální > 100k /mL. těžká trombocytopenie < 20k /mL (spontální krvácení) Mean platelet volume (MPV) fL. Aggregometrie. Klasifikace kongenitálních trombocytopatií. Agregace je indukovaná v PRP nebo v PB odebrané do citrátu sodného (ACD) přidáním aktivátoru (ADP, trombin, collagen) EDTA - induced PLT clumping - result in low PLT count. - is an artifact which should be excluded by the peripheral blood smear evaluation and repetition of PLT count using a blood sample collected to sodium citrate. RISTOCETIN IS ANTIBIOTICS WHICH INTERACTS WITH THE GP Ib ON THE PLT SURFACE AND WITH vWF IN PLASMA TO INDUCE CONFORMATION CHANGES WHICH ALLOW vWF TO BIND ON GP Ib WHICH LEADS TO AGGREGATION (MOST vWD EXCEPT TYPE 2B). some hereditary thrombocytopaties have large PLT. PLT LABORATORY.")
31
Agregace destiček

32
Platelet aggregation test - ADP agonist
Patient (Blue) shows an initial wave of aggregation followed by disaggregation beginning at 1 minute. Patient ADP release (Black) is 0 . The control PRP shows 75% aggregation (Red) The control PRP shows 1.3 uM ADP release (Green). 70 year old male with a history of coronary heart disease was scheduled for an elective inguinal hernia repair.His medications included daily aspirin and clopidogrel (Plavix) but he had stopped these 5 days previously as instructed. Platelet aggregation studies were requested to assess for residual drug-related platelet function inhibition. His platelet count was 208,000/ul. The image shown is the aggregation pattern and ADP release at a final concentration of 5uM ADP using platelet-rich plasma (PRP)from the patient and a normal control. PLAVIX (clopidogrel bisulfate) is an inhibitor of ADP-induced platelet aggregation acting by direct inhibition of adenosine diphosphate (ADP) binding to its receptor and of the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex.
 shows an initial wave of aggregation followed by disaggregation beginning at 1 minute. Patient ADP release (Black) is 0 . The control PRP shows 75% aggregation (Red) The control PRP shows 1.3 uM ADP release (Green). 70 year old male with a history of coronary heart disease was scheduled for an elective inguinal hernia repair.His medications included daily aspirin and clopidogrel (Plavix) but he had stopped these 5 days previously as instructed. Platelet aggregation studies were requested to assess for residual drug-related platelet function inhibition. His platelet count was 208,000/ul. The image shown is the aggregation pattern and ADP release at a final concentration of 5uM ADP using platelet-rich plasma (PRP)from the patient and a normal control. PLAVIX (clopidogrel bisulfate) is an inhibitor of ADP-induced platelet aggregation acting by direct inhibition of adenosine diphosphate (ADP) binding to its receptor and of the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex.")
33
Destičky a von Willebrand factor
Průtoková cytometrie - měření destičkových receptorů a aktivace destiček Protilátky proti destičkám - diagnoza autoimunitních trombocytopenií Funkční test: Ristocetin-induces PLT agglutination: u vWD se snižuje RISTOCETIN IS ANTIBIOTICS WHICH INTERACTS WITH THE GP Ib ON THE PLT SURFACE AND WITH vWF IN PLASMA TO INDUCE CONFORMATION CHANGES WHICH ALLOW vWF TO BIND ON GP Ib WHICH LEADS TO AGGREGATION (MOST vWD EXCEPT TYPE 2B).
.")
34
Model of von Willebrand Factor–Factor VIII Complex in Plasma
Figure 2. Model of von Willebrand Factor–Factor VIII Complex in Plasma. Von Willebrand factor circulates as a complex with factor VIII, thereby protecting factor VIII from degradation by the naturally occurring anticoagulant-activated protein C and localizing factor VIII at the site of vascular injury. Each mature von Willebrand factor subunit (domains D', D3, A1, A2, A3, D4, B, C1, C2, CK) dimerizes through disulfide bonds (shown as S–S) near the carboxy terminus (C). Each dimer further multimerizes through disulfide bonds near the amino terminus (N). Factor VIII (domains A1, A2, B, A3, C1, C2) is cleaved before secretion and binds to von Willebrand factor as a heterodimer. The acidic region (cross-hatching) of the A3 domain of factor VIII and the carboxy-terminal region on the C2 domain bind (noncovalent bonds are shown as dotted lines) in the amino-terminal region of the von Willebrand factor subunit (domain D'–D3). The A1 and A2 domains of the heavy chain of factor VIII are noncovalently bonded to the A3 domain of the light chain (dotted lines). At the bottom of the figure, areas of the von Willebrand factor subunit involved in the interaction with collagen and platelet glycoproteins Iba (GpIb a) and a IIb b3 are shown.
 dimerizes through disulfide bonds (shown as. S–S) near the carboxy terminus (C). Each dimer further multimerizes through disulfide bonds near the amino terminus. (N). Factor VIII (domains A1, A2, B, A3, C1, C2) is cleaved before secretion and binds to von Willebrand factor as a heterodimer. The acidic region (cross-hatching) of the A3 domain of factor VIII and the carboxy-terminal region on the C2. domain bind (noncovalent bonds are shown as dotted lines) in the amino-terminal region of the von Willebrand factor. subunit (domain D –D3). The A1 and A2 domains of the heavy chain of factor VIII are noncovalently bonded to the A3. domain of the light chain (dotted lines). At the bottom of the figure, areas of the von Willebrand factor subunit involved. in the interaction with collagen and platelet glycoproteins Iba (GpIb a) and. a IIb b3 are shown.")
35
Simplified Model of von Willebrand Factor Functions in Platelet-Plug Formation.
Figure 1. Simplified Model of von Willebrand Factor Functions in Platelet-Plug Formation. In the intact vessel wall (Panel A), endothelial cells hamper the interactions of circulating platelets and their membrane glycoproteins Ib with von Willebrand factor and collagen fibrils localized in the subendothelial extracellular matrix. When the vessel wall is intact and blood flow is normal, plasma von Willebrand factor that is present in a coiled structure and platelets coexist in circulating blood with minimal interactions. In the damaged vessel wall (Panel B), collagen and von Willebrand factor of the subendothelial matrix become exposed to flowing blood and shear forces. Plasma von Willebrand factor efficiently binds to exposed collagen and uncoils its structure, supporting the adhesion of circulating platelets in synergy with collagen. Bound von Willebrand factor interacts, at first, only with the platelet receptor GpIb and platelet tethering occurs. This interaction has a fast dissociation rate, and platelets tethered to the vessel wall still move in the direction of flow (rolling). In this interaction, collagen receptors GpVI and 1 bind to collagen and promote platelet adhesion and activation in synergy with the von Willebrand factor–GpIb interactions. Once platelets are activated (represented by irregular margins), a conformational change of 3 enhances its affinity for the ligand von Willebrand factor (receptors are shown as yellow crosses). This event, together with the rolling of platelets due to the von Willebrand factor–GpIb 3 is also responsible for platelet-to-platelet interactions that eventually lead to platelet-plug formation mediated by von Willebrand factor and, at slow flow conditions, by fibrinogen (not shown).
, endothelial cells hamper. the interactions of circulating platelets and their. membrane glycoproteins Ib. with von Willebrand factor and collagen fibrils localized. in the subendothelial extracellular matrix. When the vessel. wall is intact and blood flow is normal, plasma von. Willebrand factor that is present in a coiled structure and. platelets coexist in circulating blood with minimal interactions. In the damaged vessel wall (Panel B), collagen. and von Willebrand factor of the subendothelial matrix. become exposed to flowing blood and shear forces. Plasma. von Willebrand factor efficiently binds to exposed. collagen and uncoils its structure, supporting the adhesion. of circulating platelets in synergy with collagen. Bound von Willebrand factor interacts, at first, only with. the platelet receptor GpIb. and platelet tethering occurs. This interaction has a fast dissociation rate, and platelets. tethered to the vessel wall still move in the direction of. flow (rolling). In this interaction, collagen receptors. GpVI and 1 bind to collagen and promote platelet. adhesion and activation in synergy with the von Willebrand. factor–GpIb interactions. Once platelets are activated. (represented by irregular margins), a conformational. change of 3 enhances its affinity for the. ligand von Willebrand factor (receptors are shown as yellow. crosses). This event, together with the rolling of. platelets due to the von Willebrand factor–GpIb. 3 is also responsible for platelet-to-platelet. interactions that eventually lead to platelet-plug formation. mediated by von Willebrand factor and, at slow. flow conditions, by fibrinogen (not shown).")
36
vWd - Platelet aggregation test with Ristocetin
Platelet aggregation pattern with 1.5mg/dL Ristocetin. normal (red) plasma patient (blue) plasma Patient had a normal aPTT, factor VIII activity of 77%, vWf antigen of 61%, Ristocetin co-factor activity of <12.5% and a vWf multimer pattern showing absence of high molecular weight multimers. Differential diagnosis was vWD type 2b versus platelet-type (psedo) VWD. The ristocetin cofactor test is the primary assay used to diagnose von Willebrand disease as it measures plasma von Willebrand factor activity.
 plasma. patient (blue) plasma. Patient had a normal aPTT, factor VIII activity of 77%, vWf antigen of 61%, Ristocetin co-factor activity of <12.5% and a vWf multimer pattern showing absence of high molecular weight multimers. Differential diagnosis was vWD type 2b versus platelet-type (psedo) VWD. The ristocetin cofactor test is the primary assay used to diagnose von Willebrand disease as it measures plasma von Willebrand factor activity.")
37
von Willebrand factor protein multimer analysis on agarose gel electrophoresis
Lane 1 - normal control plasma: High molecular weight forms at the top; low molecular weight forms at the bottom. Lane 2 - Type 2B (for illustration): High molecular weight multimers are absent. Lane 3 - patient with acquired von Willebrand syndrome (AVWS) secondary to ET. Note both high and intermediate molecular weight multimers are absent.
: High molecular weight multimers are absent. Lane 3 - patient with acquired von Willebrand syndrome (AVWS) secondary to ET. Note both high and intermediate molecular weight multimers are absent.")
38
Stanovení času krvácení (Duke 1910; Ivy 1941)
Čas potřebný ke spontálnímu zastavení krvácení ze standardního poranění Funkční test primární hemostázy Duke : Měří se čas potřebný pro spontánní zastavení krvácení ze standardního vpichu do ušního lalůčku (2 - 5 min) Ivy: Měří se čas potřebný pro spontánní zastavení krvácení ze standardního řezu na předloktí Pro stanovení času krvácení se používají jednorázové lancety s pružinou, které po přiložení na předloktí a odjištění provedou automaticky standardní řez (Simplate systém). Standardnost provedení se zvyšuje umístěním tonometrické manžety nafouknuté na 40mmHg nad místo řezu.
 Ivy: Měří se čas potřebný pro spontánní zastavení krvácení ze standardního řezu na předloktí. Pro stanovení času krvácení se používají jednorázové lancety s pružinou, které po přiložení na předloktí a odjištění provedou automaticky standardní řez (Simplate systém). Standardnost provedení se zvyšuje umístěním tonometrické manžety nafouknuté na 40mmHg nad místo řezu.")
39
Stanovení času krvácení (Ivy 1941)
Prodloužený čas: poruchu funkce destiček těžkou trombocytopenii (< /uL) vonWillebrandovu chorobu (kvant. nebo kval. změny vWf) aspirin (>5 days) TEMPLATE BLEEDING TIME Normal Value: 2-7 minutes Principle: A bleeding time, which depends on hemostasis in a Clinical Significance: The bleeding time is a test for abnormalities in the platelet and vascular phases of coagulation. The relationship of bleeding time to platelet count can be of help in determining platalet function (see diagram). Manžeta tonometru nafouknutá na 40 mm Hg Řez 6x1 mm Normální hodnota min.
 vonWillebrandovu chorobu (kvant. nebo kval. změny vWf) aspirin (>5 days) TEMPLATE BLEEDING TIME. Normal Value: 2-7 minutes Principle: A bleeding time, which depends on hemostasis in a Clinical Significance: The bleeding time is a test for abnormalities in the platelet and vascular phases of coagulation. The relationship of bleeding time to platelet count can be of help in determining platalet function (see diagram). Manžeta tonometru nafouknutá na 40 mm Hg. Řez 6x1 mm. Normální hodnota min.")
40
Bleeding time is inversely related to circulating platelet count
The bleeding time is inversely related to circulating platelet count in patients with thrombocytopenia owing to decreased production (closed circles, which also include 8 normal subjects) when the count is between 100,000 per ml and 10,000 per ml. Platelet function defects are represented by subjects taking aspirin (open circles) and patients with uremia (closed triangles) and inherited severe von Willebrand disease (open triangles). Many patients with idiopathic thrombocytopenic purpura have platelets with increased hemostatic competence (open squares). Harker LA. Slichter SJ. NEJM. 287(4):155-9, 1972.
 when the count is between 100,000 per ml and 10,000 per ml. Platelet function defects are represented by subjects taking aspirin (open circles) and patients with uremia (closed triangles) and inherited severe von Willebrand disease (open triangles). Many patients with idiopathic thrombocytopenic purpura have platelets with increased hemostatic competence (open squares). Harker LA. Slichter SJ. NEJM. 287(4):155-9,")
41
Stanovení rezistence kapilár (Rumpel, Leede)
Zjisťuje se počet petechií, které se vytvoří na určité ploše předloktí (4x4 cm) po stlačení známou silou (manžeta 10,5 kPa/10 min) nebo po aplikaci podtlaku (Brown, 1949). V klasickém uspořádání počet petechií > 5 signalizuje zvýšení fragility kapilár. Diagnotika hereditárních purpur (Weber-Rendu-Osler).
 po stlačení známou silou (manžeta 10,5 kPa/10 min) nebo po aplikaci podtlaku (Brown, 1949). V klasickém uspořádání počet petechií > 5 signalizuje zvýšení fragility kapilár. Diagnotika hereditárních purpur (Weber-Rendu-Osler).")
42
PLAZMATICKÝ KOAGULAČNÍ SYSTÉM

43
Clotting Process Initiating the Clotting Process
Damaged cells display a surface protein called tissue factor (TF) that binds to activated Factor 7 (TF-7) to cleave: Factor 10 2. Factor 10 binds and activates Factor 5 (prothrombinase) convertíng prothrombin (also known as Factor II) to thrombin 3. Thrombin proteolytically cleave fibrinogen (Factor I) to fibrin. 4. Factor 13 forms covalent bonds between the soluble fibrin molecules converting them into an insoluble meshwork — the clot.
 that binds to activated Factor 7 (TF-7) to cleave: Factor Factor 10 binds and activates Factor 5 (prothrombinase) convertíng prothrombin (also known as Factor II) to thrombin. 3. Thrombin proteolytically cleave fibrinogen (Factor I) to fibrin. 4. Factor 13 forms covalent bonds between the soluble fibrin. molecules converting them into an insoluble meshwork — the clot.")
44
Vyšetření PKS Krev odebraná do citrátu sodného se odstředí
Získá se tak citrátová plazma chudá na destičky (PPP), která se použije k testu.
, která se použije k testu.")
45
Prothrombin time (PT): Reference range 11-14 seconds; INR 1.0-1.3
A. Principle: Plasma, obtained from blood to which a calcium-binding anticoagulant (citrate) has been added, will clot in a few seconds when recalcified in the presence of tissue factor. The elapsed time between the addition of calcium-tissue factor mixture and the presence of a detectable clot is the prothrombin time. In order to standardize the monitoring of oral anticoagulation among laboratories, the International Normalized Ratio (INR) was developed to compensate for the wide variation among reagent and instrument systems. The sensitivity of a reagent used with an instrument is compared to an international standard. The relationship of the test system to the standard, the International Sensitivity Index (ISI), is determined. The INR of the patient can then be calculated by the formula: INR= (PTpat/PTcont)ISI Where PTpat is the protime of the patient and PT the mean of 20 normal patient protimes. B. Clinical Significance: The prothrombin time measures the clotting time of plasma in the presence of an optimal concentration of tissue extract and serves as an indicator of the overall efficiency of the extrinsic clotting system. The prothrombin time may be prolonged in: inherited deficiencies of factors I, II, V, VII, and X; acquired multiple deficiencies of II, VII and X in coumarin-type anticoagulant therapy in which the target of anticoagulation is an INR of 2 to 3 in most clinical settings; parenchymal liver disease; vitamin K deficiency; disseminated intravascular clotting and fibrinolysis. Most reagents used for doing the prothrombin time contain an inhibitor of heparin, therefore the test does not reflect the presence of heparin in the specimen.
 has been added, will clot in a few seconds when recalcified in the presence of tissue factor. The elapsed time between the addition of calcium-tissue factor mixture and the presence of a detectable clot is the prothrombin time. In order to standardize the monitoring of oral anticoagulation among laboratories, the International Normalized Ratio (INR) was developed to compensate for the wide variation among reagent and instrument systems. The sensitivity of a reagent used with an instrument is compared to an international standard. The relationship of the test system to the standard, the International Sensitivity Index (ISI), is determined. The INR of the patient can then be calculated by the formula: INR= (PTpat/PTcont)ISI. Where PTpat is the protime of the patient and PT the mean of 20 normal patient protimes. B. Clinical Significance: The prothrombin time measures the clotting time of plasma in the presence of an optimal concentration of tissue extract and serves as an indicator of the overall efficiency of the extrinsic clotting system. The prothrombin time may be prolonged in: inherited deficiencies of factors I, II, V, VII, and X; acquired multiple deficiencies of II, VII and X in coumarin-type anticoagulant therapy in which the target of anticoagulation is an INR of 2 to 3 in most clinical settings; parenchymal liver disease; vitamin K deficiency; disseminated intravascular clotting and fibrinolysis. Most reagents used for doing the prothrombin time contain an inhibitor of heparin, therefore the test does not reflect the presence of heparin in the specimen.")
46
Protrombinový čas PT (Quickův test) test simuluje hlavní cestu aktivace PKS cestu tkáňového faktoru (extrinsic pathway) Do citrátové plazmy se přidá přebytek tkáňového tromboplastinu (tkáňový faktor v negativně nabitých fosfolipidech) a CaCl2. V koagulometru se měří čas vzniku fibrinového vlákna. Normální hodnoty: PTN= s Prodloužení PT: deficit FV nebo vit. K dep. FII, VII, X těžký deficit FBG, vysoké FDP, porucha konverze FBG, v určitém uspořádání není ovlivněn heparinem (do 1 U/mL)
 a CaCl2. V koagulometru se měří čas vzniku fibrinového vlákna. Normální hodnoty: PTN= s. Prodloužení PT: deficit FV nebo vit. K dep. FII, VII, X. těžký deficit FBG, vysoké FDP, porucha konverze FBG, v určitém uspořádání není ovlivněn heparinem (do 1 U/mL)")
47
Protrombinový čas PT (Quickův test) test simuluje hlavní cestu aktivace PKS
Využití testu: screeningový test řízení orální antikoagulační terapie antagonisty vit. K test jaterní proteosyntézy (FVII) Vyjadřování výsledků: Mezinárodní normalizovaný poměr (INR) INR= (PTP/ PTN)ISI ISI = mezinárodní index senzitivity užitého tromboplastinu (většinou > 1). INR je oficiálně určen pouze pro řízení orální antikoagulační terapie (max. terapeut. INR = 4,5), používá se však často všeobecně RAISED TO ISI POWER
 Vyjadřování výsledků: Mezinárodní normalizovaný poměr (INR) INR= (PTP/ PTN)ISI. ISI = mezinárodní index senzitivity užitého tromboplastinu (většinou > 1). INR je oficiálně určen pouze pro řízení orální antikoagulační terapie (max. terapeut. INR = 4,5), používá se však často všeobecně. RAISED TO ISI POWER.")
48
RAISED TO ISI POWER

50
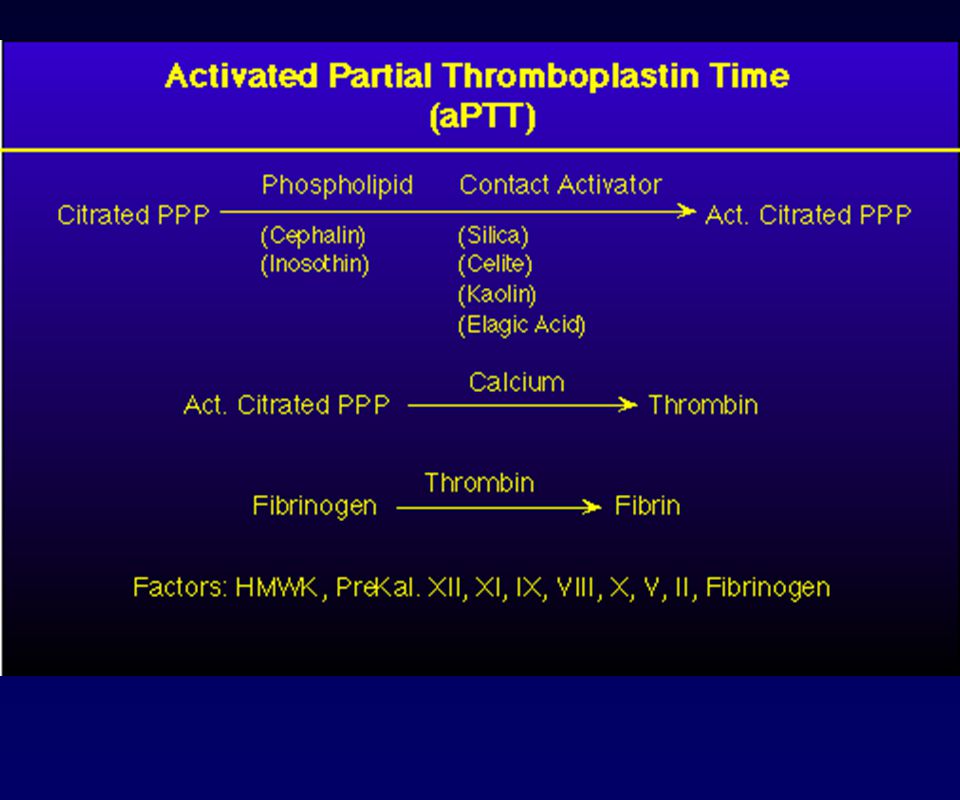
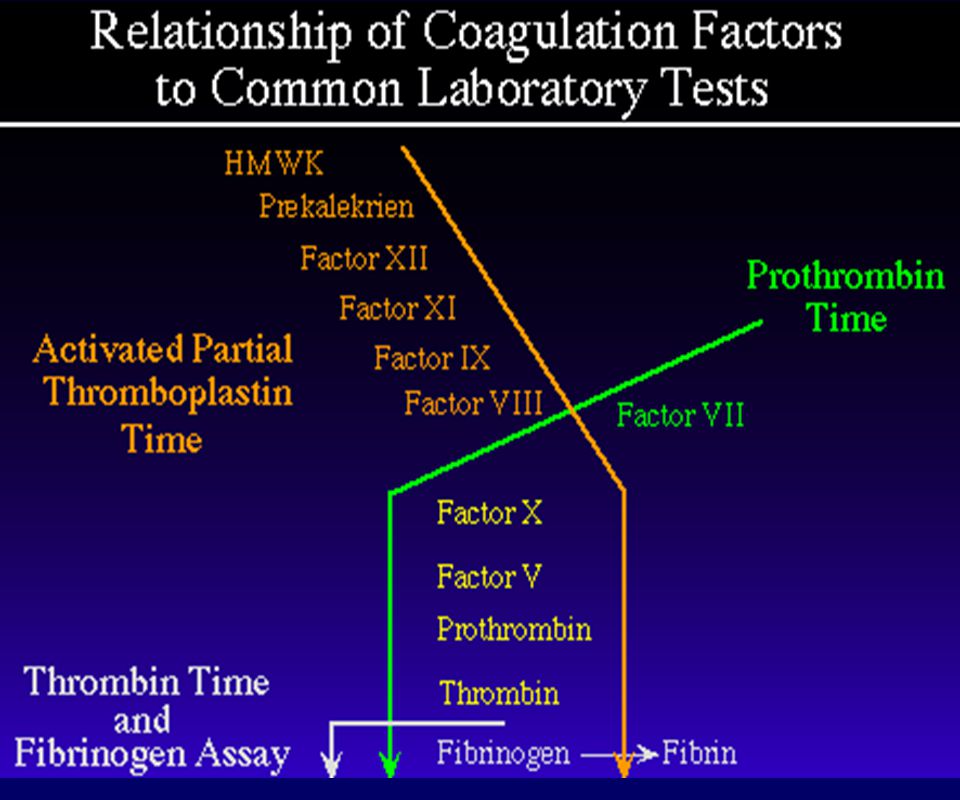
Aktivovaný parciální tromboplastinový čas APTT test simuluje kontaktní cestu aktivace PKS (vnitřní cestu) Do citrátové plazmy se aplikuje kontaktní aktivátor (např.kaolin) pro aktivaci kontaktního systému a negativně nabité fosfolipidy pro umožnění tvorby FX- a FII- aktivačních komplexů. Plazma se rekalcifikuje CaCl2 a v koagulometru se měří čas do vzniku fibrinového vlákna. Normální hodnoty: APTTN = s Využití testu: screeningový test, diagnostika deficitu faktorů “vnitřního“ systému, lupus antikoagulans, řízení heparinové terapie.
 pro aktivaci kontaktního systému a negativně nabité fosfolipidy pro umožnění tvorby FX- a FII- aktivačních komplexů. Plazma se rekalcifikuje CaCl2 a v koagulometru se měří čas do vzniku fibrinového vlákna. Normální hodnoty: APTTN = s. Využití testu: screeningový test, diagnostika deficitu faktorů vnitřního systému, lupus antikoagulans, řízení heparinové terapie.")
51
Aktivovaný parciální tromboplastinový čas APTT test simuluje kontaktní cestu aktivace PKS (vnitřní cestu) Prodloužení APTT: deficit FII,V, X, deficit kontaktních faktorů - F XII, PK, HMWK, deficit FXI, FIX , FVIII (hemofilie C, B,A) lupus antikoagulans těžkýdeficit FBG vysoké FDP porucha konverze FBG Zkrácení APTT: protrombotický stav Vyjadřování výsledků: APTT pacienta, APTT kontroly (normálu), Při heparinové terapii řízené APTT požadováno 1,5x - 2,5 x prodloužení.
 lupus antikoagulans. těžkýdeficit FBG. vysoké FDP. porucha konverze FBG. Zkrácení APTT: protrombotický stav. Vyjadřování výsledků: APTT pacienta, APTT kontroly (normálu), Při heparinové terapii řízené APTT požadováno 1,5x - 2,5 x prodloužení.")
52
PT PTT Acquired Disorder Congenital Disorder Long Normal Liver disease or vitamin K deficiency Factor VII deficiency Acquired factor VIII inhibitor Factor VIII, IX, or XI deficiency DIC, liver disease, Lupus anticoagulant (LA) Fibrinogen, prothrombin, factor V or X deficiency Thrombocytopenia, qualitative platelet disorder Mild factor deficiency, mild von Willebrand disease, factor XIII deficiency
 Fibrinogen, prothrombin, factor V or X deficiency. Thrombocytopenia, qualitative platelet disorder. Mild factor deficiency, mild von Willebrand disease, factor XIII deficiency.")
53
Ostatní vyšetření PKS FBG - stanovení concentrace fibrinogenu v plazmě (normál : g/L). Funkční (klotabilní FBG) nebo imunologická metoda Hypofibrinogenemie (např. při akutní DIC) Hyperfibrinogenemie ( při zánětu, protein akutní fáze) TT - trombinový čas plazmy (normál s). Přímé vyšetření konverze FBG na fibrin Prodloužen: dysfibrinogenemii, těžké hypo- afibrinogenemii vysoké hladině FDP (působí antipolymeračně) při heparinové terapii
 nebo imunologická metoda. Hypofibrinogenemie (např. při akutní DIC) Hyperfibrinogenemie ( při zánětu, protein akutní fáze) TT - trombinový čas plazmy (normál s). Přímé vyšetření konverze FBG na fibrin. Prodloužen: dysfibrinogenemii, těžké hypo- afibrinogenemii. vysoké hladině FDP (působí antipolymeračně) při heparinové terapii.")
54
Speciální vyšetření PKS
Vyšetření aktivity jednotlivých faktorů PKS pomocí APTT testu s použitím selektivně deficitní plazmy - diagnostika hemofilie A (FVIII), B(FIX), C (FXI) a dalších deficiencí.
, B(FIX), C (FXI) a dalších deficiencí.")
55
Mixing Study (1:1 mix of patient and normal plasma):
When the aPTT is prolonged, information on the possible etiology of the abnormality can be obtained by performing the mixing study. In brief, an equal portion of normal and patient plasma are mixed together and the aPTT is repeated on the mixture. If the resulting time is within the reference range, then it is likely that the prolonged aPTT is due to a deficiency of coagulation factor. If the resulting time is beyond the reference range, then the prolonged aPTT is likely to be due to an inhibitor of coagulation (a medication like heparin or antibody). This is due to the fact that no aPTT test will detect (is sensitive to) deficiency of a coagulation factor at the level of 50% . Because of the mix with normal plasma, the resulting mixture will have at least 50% of all factors, even if the patient value is 0%. Distinction between deficiency and inhibitor is an important step in determining there as on for the original prolonged time. It is important remember that some antibodies may take some time to bind to their respective antigen. Thus, if the original mixing study results in correction into the reference range, then an incubated mix is indicated . The principle is depicted in the figure. The incubation time is generally 1-2 hours at 37 degrees C. The purpose of the incubation in to increase the sensitivity of the test ,it does not provide information concerning the cause (specificity) of the test. An algorithm for the evaluation of the prolonged aPTT is depicted in the figure . In general, mixing studies to evaluate a long PT are not useful. If both PT and aPTT are prolonged, pursuit of the long aPTT should be sufficient. If the PT is abnormal with a normal aPTT, the problem is with factor VII and inhibition of factor VII is extremely rare.
. This is due to the fact that no aPTT test will detect (is sensitive to) deficiency of a coagulation factor at the level of 50% . Because of the mix with normal plasma, the resulting mixture will have at least 50% of all factors, even if the patient value is 0%. Distinction between deficiency and inhibitor is an important step in determining there as on for the original prolonged time. It is important remember that some antibodies may take some time to bind to their respective antigen. Thus, if the original mixing study results in correction into the reference range, then an incubated mix is indicated . The principle is depicted in the figure. The incubation time is generally 1-2 hours at 37 degrees C. The purpose of the incubation in to increase the sensitivity of the test ,it does not provide information concerning the cause (specificity) of the test. An algorithm for the evaluation of the prolonged aPTT is depicted in the figure . In general, mixing studies to evaluate a long PT are not useful. If both PT and aPTT are prolonged, pursuit of the long aPTT should be sufficient. If the PT is abnormal with a normal aPTT, the problem is with factor VII and inhibition of factor VII is extremely rare.")
56
Metody vyšetření srážlivosti plné krve u lůžka
Lee-Whiteův test - koagulační čas plné krve odebrané bez antikoagulancí v polystyrenové nebo skleněné zkumavce při 37oC. Normální hodnoty min., dle uspořádání. Hrubý orientační test funkce PKS v akutních stavech. Trombinový čas plné krve - koagulační čas plné krve odebrané bez antikoagulancií ve zkumavce se standardním množstvím trombinu. Slouží pro rychlou orientační kontrolu přítomnosti fibrinogenu (+/-) v krvi při dekompenzaci akutní DIC. Aktivovaný koagulační čas (ACT) - krev odebraná bez antikoagulancia se aplikuje do zkumavky s kontaktním aktivátorem (silika, kaolin) a v přístroji je při 37oC míchána do odečtení času koagulace. Rutinní použití pro kontrolu heparinizace při mimotělním oběhu a hemodialýze. ACT normální krve je cca 150 s, při heparinizaci pro dlouhodobý MO nebo hemodialýzu s, při MO v kardiochirurgii > 600 s.
 v krvi při dekompenzaci akutní DIC. Aktivovaný koagulační čas (ACT) - krev odebraná bez antikoagulancia se aplikuje do zkumavky s kontaktním aktivátorem (silika, kaolin) a v přístroji je při 37oC míchána do odečtení času koagulace. Rutinní použití pro kontrolu heparinizace při mimotělním oběhu a hemodialýze. ACT normální krve je cca 150 s, při heparinizaci pro dlouhodobý MO nebo hemodialýzu s, při MO v kardiochirurgii > 600 s.")
57
Pravděpodobné výsledky laboratorních testů při různých poruchách hemostázy (I)
Porucha PLT BT APTT PT TT FBG Trombocytopenie L P N N N N Hemofilie A N N P N N N Hemofilie B N N P N N N Hemofilie C N N P N N N vW choroba N P N/P N N N LA N N P N/P N N

58
Pravděpodobné výsledky laboratorních testů při různých poruchách hemostázy (II)
Porucha PLT BT APT T PT TT FBG N N P P N N FV-def. FII-def. FVII-def. Vit.Kdef./OA FBG-def. Heparin N N N P P N N N P N N P N N P P N N N N P P P L N N/P P N N/P P

60
VÝUKOVÁ KAZUISTIKA- KOA 1
Žena, 55 let ve 26 letech, 10 dnů po III. porodu - DVT ldk, SVT pdk terapie - heparin, následně OA (warfarin) 6 měsíců v 41, 43 letech - 2 nekomplikované gyn. chirurgie (ov. cysta) v 45 letech - opak. epizody tachykardie - ECHO -mitr. stenóza v 46, 53, 54 letech - SVT dk Otázka: Jaké znáte doposud známé příčiny hereditárních a získaných trombofílií. Jaká laboratorní vyšetření navrhujete?
 6 měsíců. v 41, 43 letech - 2 nekomplikované gyn. chirurgie (ov. cysta) v 45 letech - opak. epizody tachykardie - ECHO -mitr. stenóza. v 46, 53, 54 letech - SVT dk. Otázka: Jaké znáte doposud známé příčiny hereditárních a získaných trombofílií. Jaká laboratorní vyšetření navrhujete")
61
KOA 1/II protein S aktivita 52%,
stanoven APC poměr - APTT test s a bez standardního přídavku APC. APC poměr = (APTT s APC/ APTT bez APC) = normál = 1,15 pacientka DNA analýza F V: PCR fragmentu s nukleotidem 1691, restrikční enzym Mn1 zjištěna homozygotní mutace FV:Q506 Leiden . Otázka: Jaká je úloha aktivovaného proteinu C (APC) v PKS Popište funkci systému proteinu C. Jakou poruchu u pacientky předpokládáte ? Otázka: Vysvětlete princip APC-rezistence ?
 = normál. = 1,15 pacientka. DNA analýza F V: PCR fragmentu s nukleotidem 1691, restrikční enzym Mn1 zjištěna homozygotní mutace FV:Q506 Leiden . Otázka: Jaká je úloha aktivovaného proteinu C (APC) v PKS Popište funkci systému proteinu C. Jakou poruchu u pacientky předpokládáte Otázka: Vysvětlete princip APC-rezistence")
62
KOA 1/III Regulace trombinové aktivity
HPS AT T PKS T T TF AT FVa PS FVIIIa APC Protein C systém je esenciální pro regulaci trombinové aktivity. Aktivovaný trombin (T) reaguje na povrchu endotelu s receptorem trombomodulinem (TM). Trombin v komplexu s trombomodulinem ztrácí své prokoagulační aktivity a aktivuje v plazmě přítomný protein C. Aktivovaný protein C (APC) s kofaktorem proteinem S degraduje FV a FVIII PKS a tím se zpomaluje aktivace trombinu. Je to důležitá negativní zpětná vazba aktivace trombinu. Homozygotní PC deficienti zmírají v novorozeneckém věku na těžké trombozy a DIC, heterozygoti trpí trombofilií. U 3 - 5% populace se vyskytuje mutace FV 506 Arg - Glu, a zmutovaný FV 506 Glu (Leiden) je rezistentní vuči proteolýze APC. Vzniká tak dispozice k trombofilii. HPS PC TFPI PC T TM ENDOTEL
 reaguje na povrchu endotelu s receptorem trombomodulinem (TM). Trombin v komplexu s trombomodulinem ztrácí své prokoagulační aktivity a aktivuje v plazmě přítomný protein C. Aktivovaný protein C (APC) s kofaktorem proteinem S degraduje FV a FVIII PKS a tím se zpomaluje aktivace trombinu. Je to důležitá negativní zpětná vazba aktivace trombinu. Homozygotní PC deficienti zmírají v novorozeneckém věku na těžké trombozy a DIC, heterozygoti trpí trombofilií. U 3 - 5% populace se vyskytuje mutace FV 506 Arg - Glu, a zmutovaný FV 506 Glu (Leiden) je rezistentní vuči proteolýze APC. Vzniká tak dispozice k trombofilii. HPS. PC. TFPI. PC. T. TM. ENDOTEL.")
63
KOA 1/IV U pacientky náhlé epizody atriální fibrilace, ECHO - LA trombus, mitrální stenoza Kardiochir. výkon : trombektomie a náhrada mitrální chlopně. Zahájena dlouhodobá léčba orálními antikoagulancii s udržovanou hodnotou INR = 3,5 - 4,5. Otázka: jaký je princip terapie orálními antikoagulancii? Co je to INR? Jaké budou hodnoty základních koagulačních vyšetření u pacientky ?

64
Dual Function of Native Factor V
Native FV is a 330-kD multidomain (A1-A2-B-A3-C1-C2) glycoprotein synthesized in the liver and secreted in plasma as a single-chain molecule with a dual function in the coagulation process. After limited proteolysis by thrombin at residues Arg709, Arg1018, and Arg1545, FV loses the B domain and is converted to the activated form (FVa), which is comprised of an aminoterminal heavy chain (A1-A2) and a carboxyl-terminal light chain (A3-C1-C2) held together by a noncovalent Ca2+-dependent bond. FVa promotes prothrombin activation within the prothrombinase complex and is subsequently inactivated (FVi) by the activated protein C (APC)/protein S complex via proteolytic cleavage at Arg306 and Arg506. Alternatively, native FV can be directly cleaved by APC at Arg506 to yield an as yet ill-defined anticoagulant molecule (FVac) that stimulates the APC-mediated inactivation of FVIIIa. APC-mediated cleavages of FV(a) that are suppressed by the FV Leiden mutation (FVL) are marked by a cross.
 glycoprotein. synthesized in the liver and secreted in plasma as a single-chain molecule with a. dual function in the coagulation process. After limited proteolysis by thrombin at. residues Arg709, Arg1018, and Arg1545, FV loses the B domain and is converted. to the activated form (FVa), which is comprised of an aminoterminal heavy chain. (A1-A2) and a carboxyl-terminal light chain (A3-C1-C2) held together by a. noncovalent Ca2+-dependent bond. FVa promotes prothrombin activation within. the prothrombinase complex and is subsequently inactivated (FVi) by the. activated protein C (APC)/protein S complex via proteolytic cleavage at Arg306. and Arg506. Alternatively, native FV can be directly cleaved by APC at Arg506 to. yield an as yet ill-defined anticoagulant molecule (FVac) that stimulates the. APC-mediated inactivation of FVIIIa. APC-mediated cleavages of FV(a) that are. suppressed by the FV Leiden mutation (FVL) are marked by a cross.")
Podobné prezentace