Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
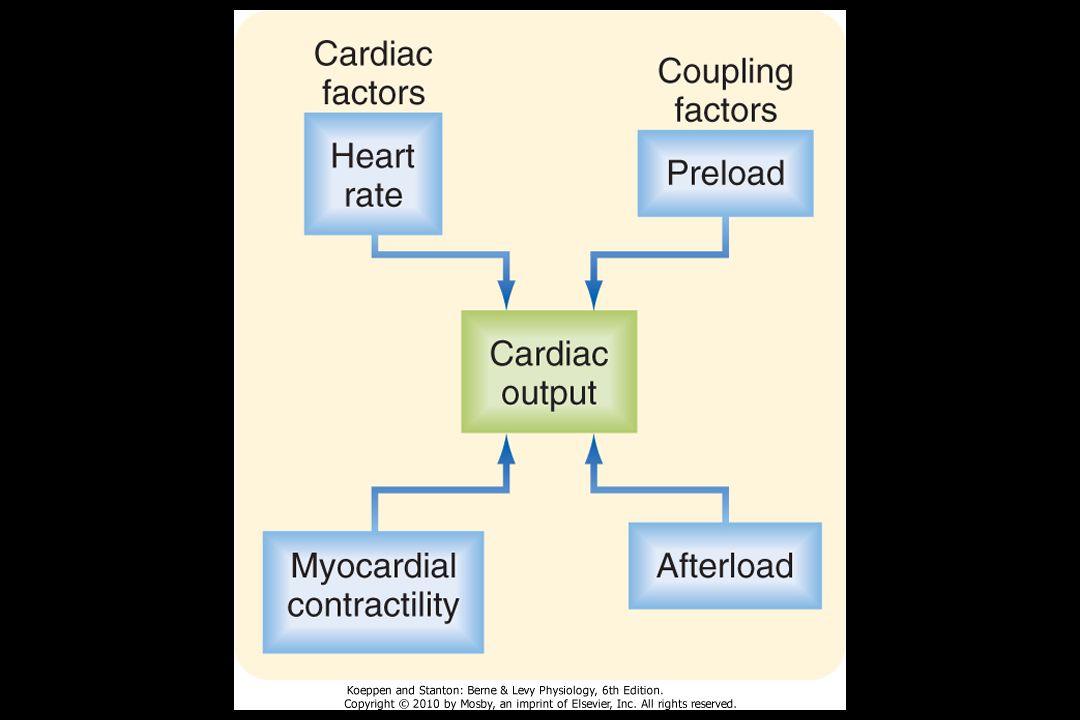
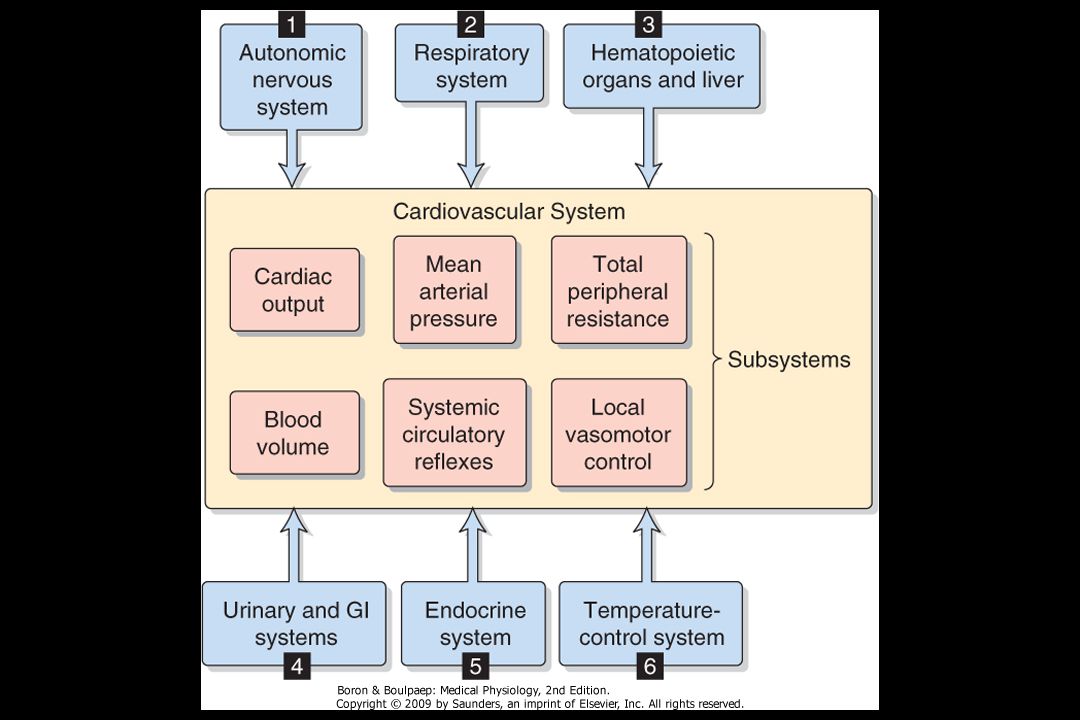
BP = CO x TPR BP = blood pressure CO = cardiac output
(stroke volume x heart rate) BP = blood pressure CO = cardiac output TPR = Total peripheral resistance
 BP = blood pressure. CO = cardiac output. TPR = Total peripheral resistance.")
5
5

9
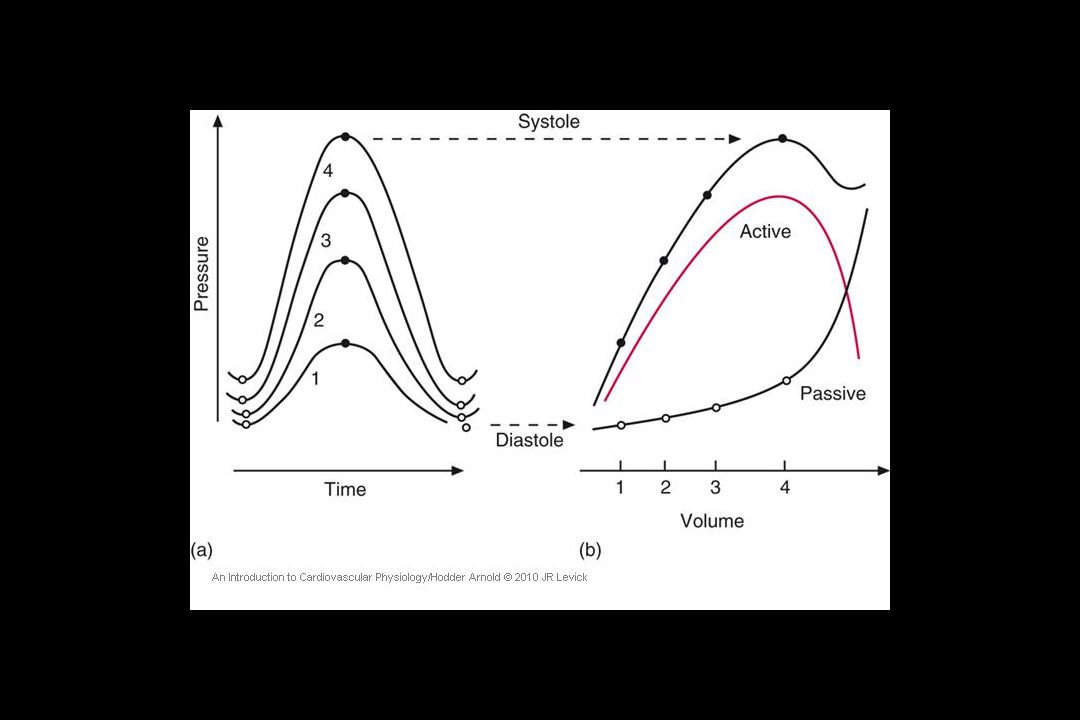
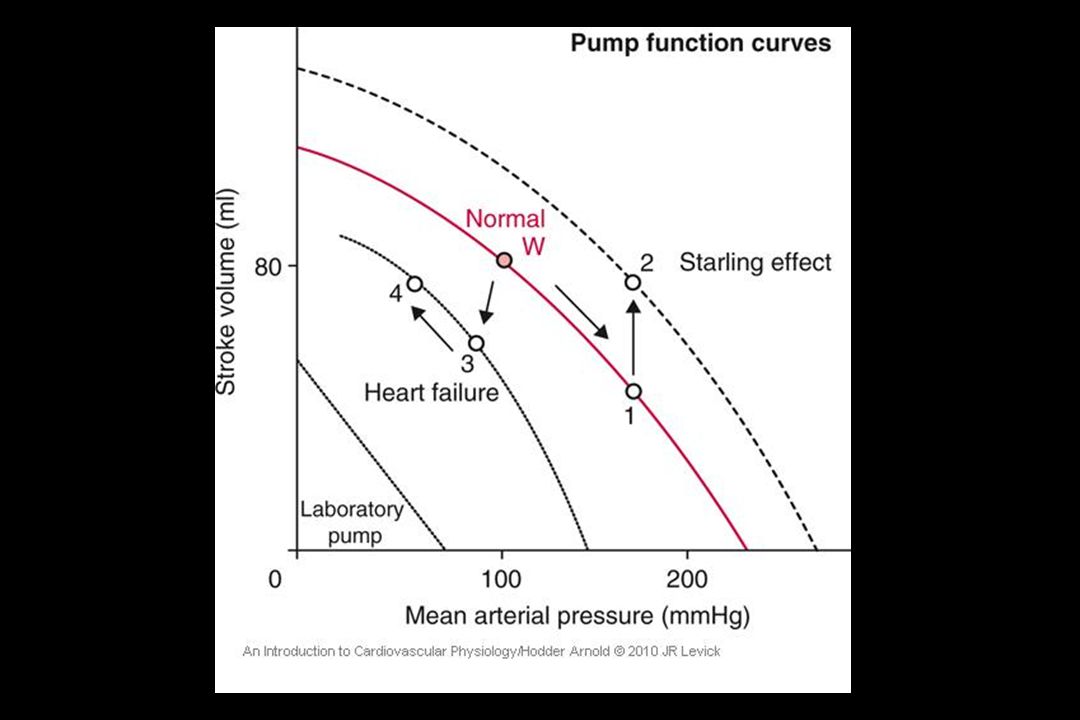
Starling’s law of the heart (1914)
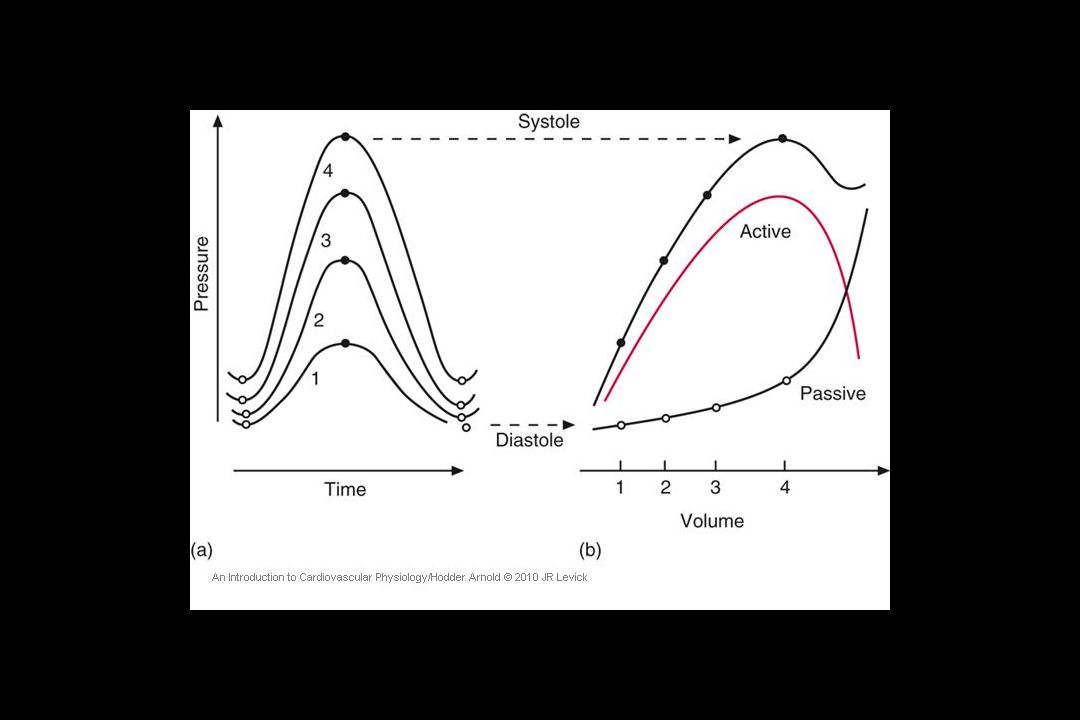
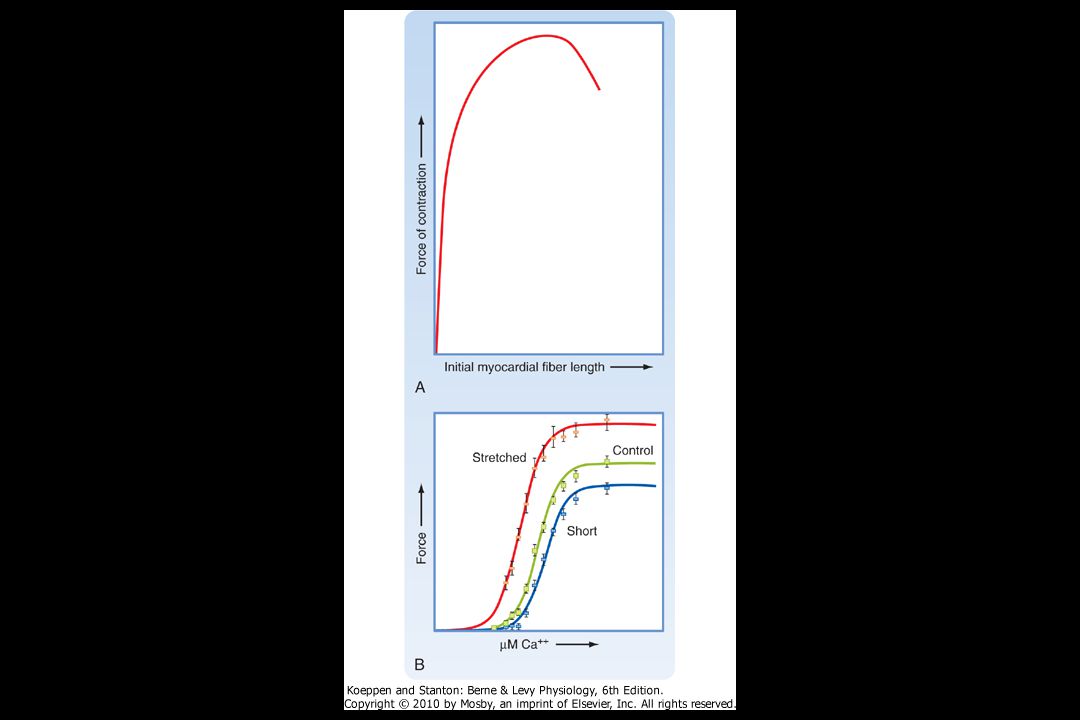
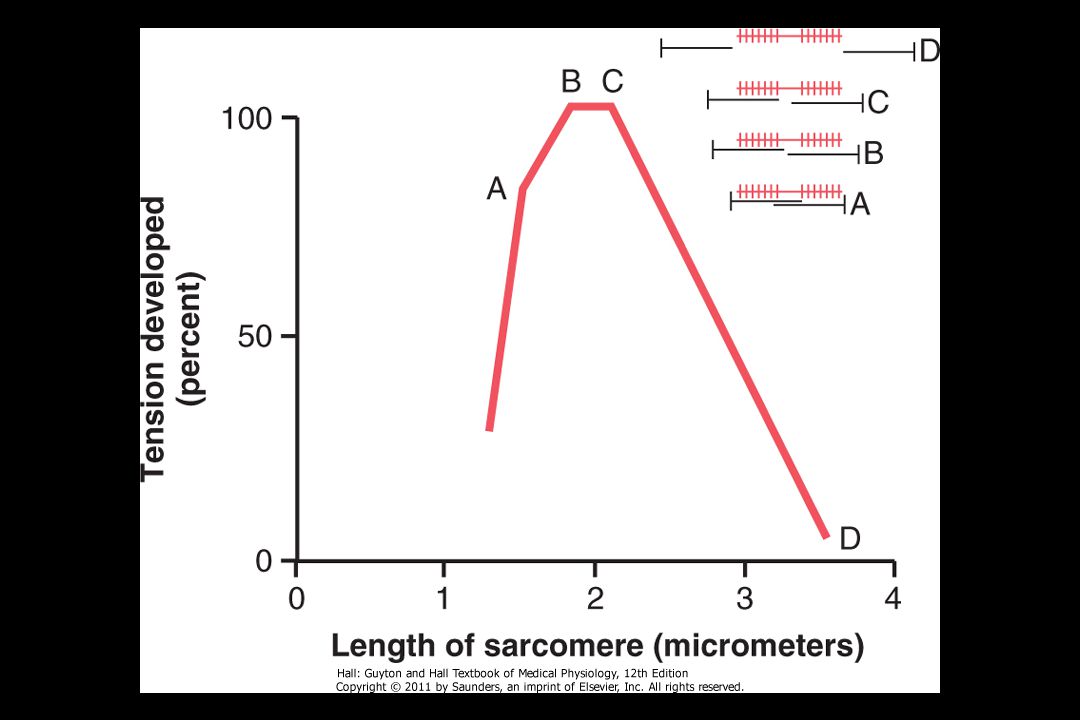
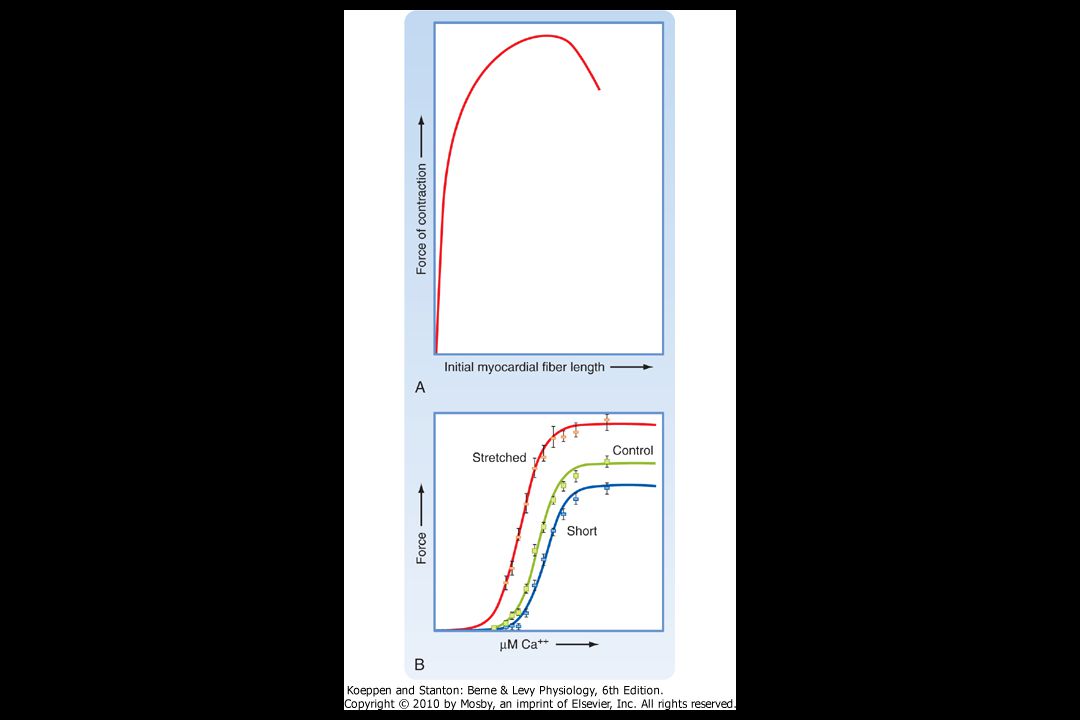
‘The energy of contraction is proportional to the muscle fibre length at rest. (Arterial pressure held constant) Stroke volume (human) ml 70 5 10 15 Ascending limb Plateau Normal, rest When the responses to lots of changes in filling pressure are plotted out, we see that the relation is a curve, called a ventricular function curve or Starling curve. Humans are normally on the rising part (‘ascending limb’) – note the typical human values. At a LV end-diastolic pressures of 10 mmHg or higher, the curve approaches a plateau i.e. there is no further gain in stroke volume with distension. At extreme, non-physiological filling pressures (possible in Starling’s isolated heart–lung experiment but probably never attained in living humans) the stroke volume falls off with increasing distension – the ‘descending limb’. This is partly due to leakage of the atrio-ventricular valves when the heart is over-distended and partly due to Laplace’s law, as explained on the next slide. Central venous pressure (mmHg) Filling pressure The ’ventricular function curve’ or ‘Starling curve’ Hodder Arnold / An Introduction to Cardiovascular Physiology © 2010 J. Rodney Levick 9
 Stroke. volume. (human) ml Ascending limb. Plateau. Normal, rest. When the responses to lots of changes in filling pressure are plotted out, we see that the relation is a curve, called a ventricular function curve or Starling curve. Humans are normally on the rising part (‘ascending limb’) – note the typical human values. At a LV end-diastolic pressures of 10 mmHg or higher, the curve approaches a plateau i.e. there is no further gain in stroke volume with distension. At extreme, non-physiological filling pressures (possible in Starling’s isolated heart–lung experiment but probably never attained in living humans) the stroke volume falls off with increasing distension – the ‘descending limb’. This is partly due to leakage of the atrio-ventricular valves when the heart is over-distended and partly due to Laplace’s law, as explained on the next slide. Central venous pressure (mmHg) Filling pressure. The ’ventricular function curve’ or ‘Starling curve’ Hodder Arnold / An Introduction to Cardiovascular Physiology © 2010 J. Rodney Levick. 9.")
10
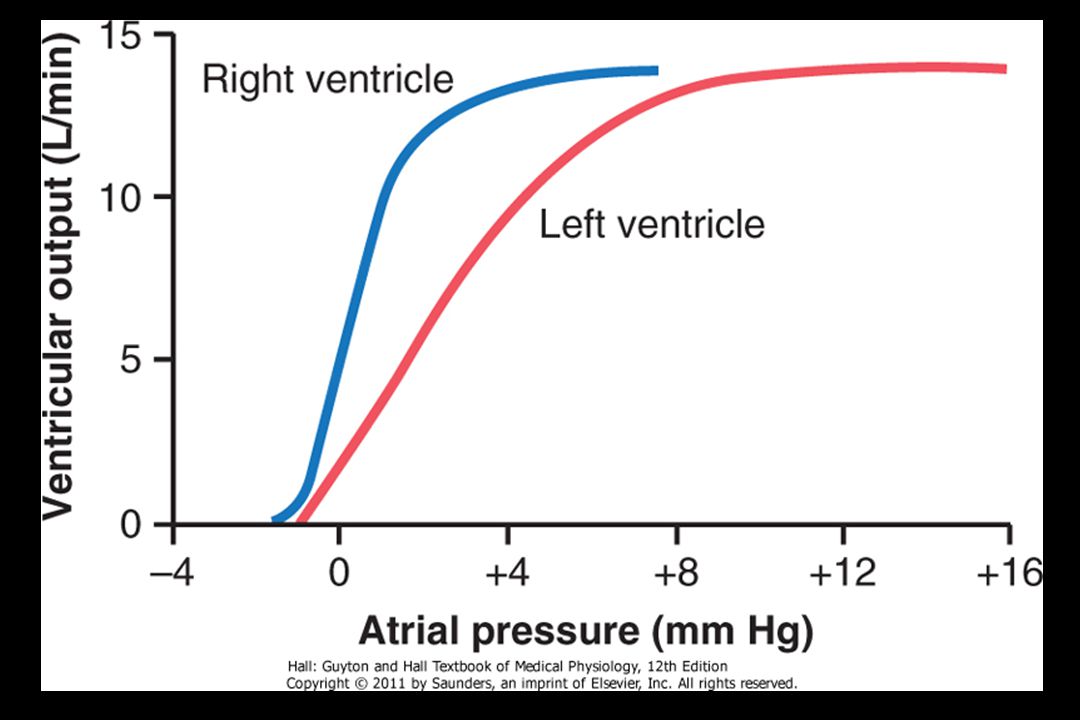
How are RV and LV stroke volumes kept equal?
The filling pressure of the left heart is determined to a large extent by the output of the right ventricle, and therefore by CVP. This slide explains how the right ventricle output influences the filling pressure of the left ventricle. Starling’s law ensures that right ventricular output equals left ventricular output over any time intervals longer than a few beats. Any prolonged imbalance would be disastrous for the volume of blood in the pulmonary circulation. Equalisation of right and left ventricular outputs is thus the single most important role of Starling’s law of the heart. 10 Hodder Arnold / An Introduction to Cardiovascular Physiology © 2010 J. Rodney Levick 10

12
12

13
13

16
P = r Increasing the radius reduces the curvature,
Laplace´s law states that, for a hollow sphere, the internal pressure (P) is proportional to the wall tension (T) and is inversely proportional to the internal radius (r): 2T P = r Tension is a force equal to wall stress (S) times Wall thickness (w): 2Sw Increasing the radius reduces the curvature, and therefore the inward component of the wall stress, so pressure falls. 16
 is proportional to the. wall tension (T) and is inversely proportional to. the internal radius (r): 2T. P = r. Tension is a force equal to wall stress (S) times. Wall thickness (w): 2Sw. Increasing the radius reduces the curvature, and therefore the inward component of the. wall stress, so pressure falls. 16.")
17
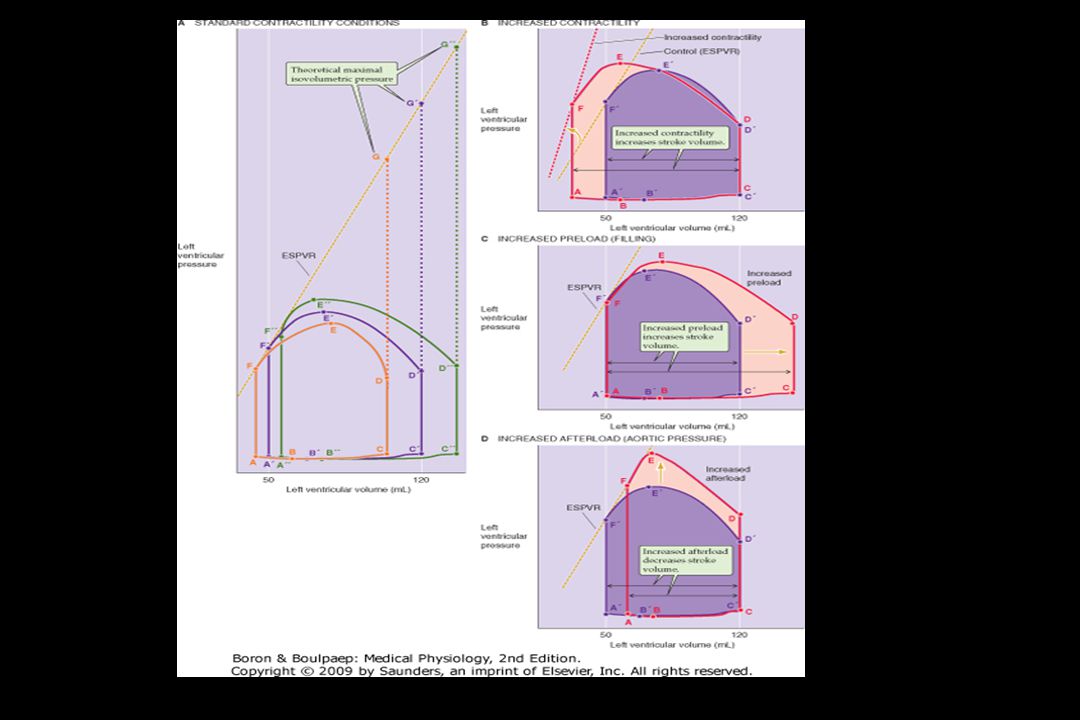
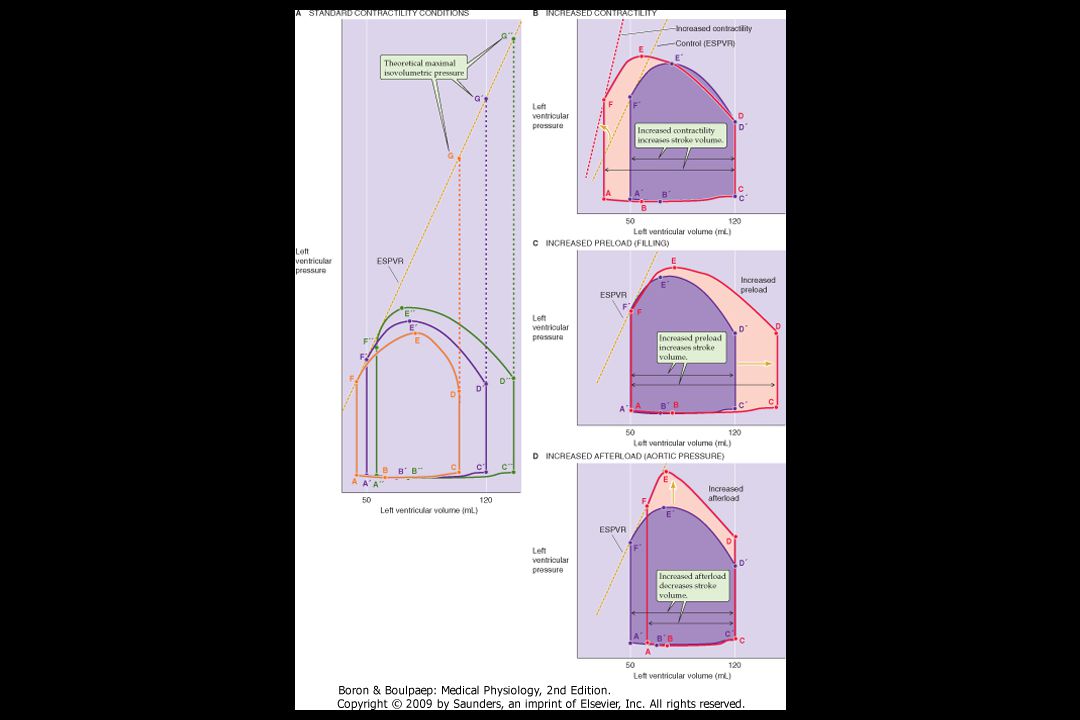
The Laplace effect and the Frank-Starling mechanism clearly have opposite effects on ventricular performance: Distension of the ventricle raises its force of contraction – due to Starling´s law X Distension also reduces the pressure generated by a given contractile force – due to Lapace´s law. Fortunately, under physiological conditions (i.e. in a healthy heart) the gain in contractile energy resulting from Moderated distension (Starling´s law) greatly outweighs the fall in pressure-generating efficiency (Laplace´s law) In contrast, the failing heart is often grossly dilated, making the Laplace effect the dominant one. An increase in radius in an already swollen heart causes little to no increase in contractile force, because the ventricle is on the plateau of the Starling curve, but the increase in radius impairs the generation of systolic pressure and hence ejection (Laplace´s law). Reduction of cardiac distension is an important therapeutic goal in heart failure
 the gain in contractile energy resulting from. Moderated distension (Starling´s law) greatly outweighs the fall in pressure-generating efficiency (Laplace´s law) In contrast, the failing heart is often grossly dilated, making the Laplace effect the dominant one. An increase in radius in an already swollen heart causes little to no increase in contractile force, because the ventricle is on the plateau of the Starling curve, but the increase in radius impairs. the generation of systolic pressure and hence ejection (Laplace´s law). Reduction of cardiac distension is an important therapeutic goal in heart failure.")
20
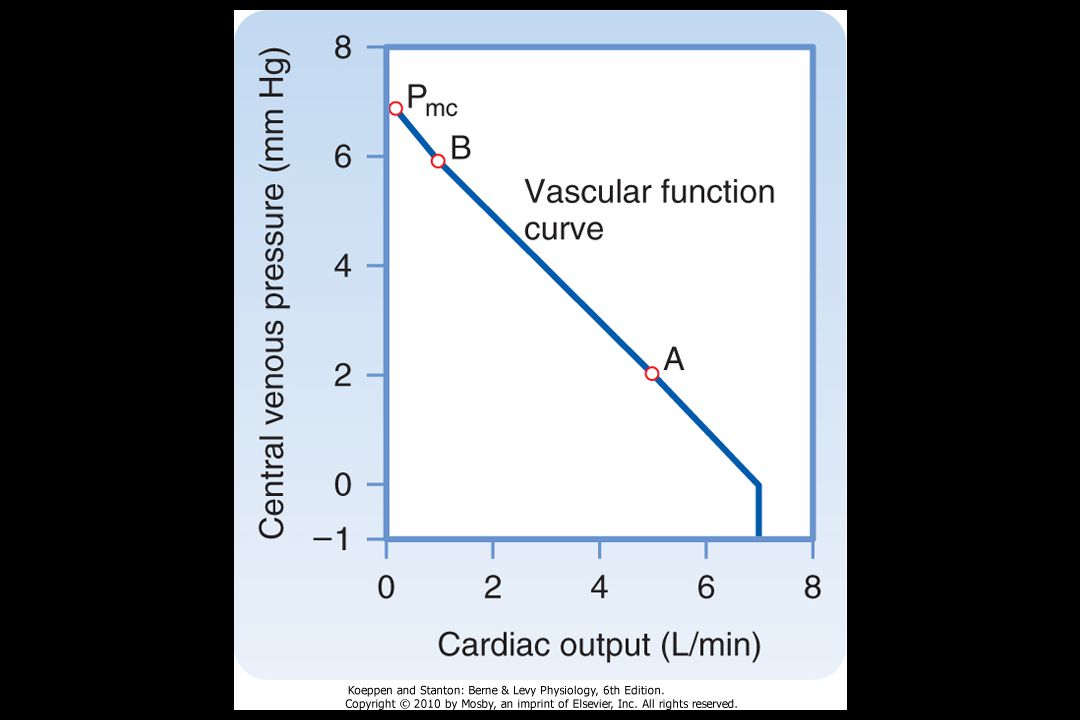
CVP = central venous pressure
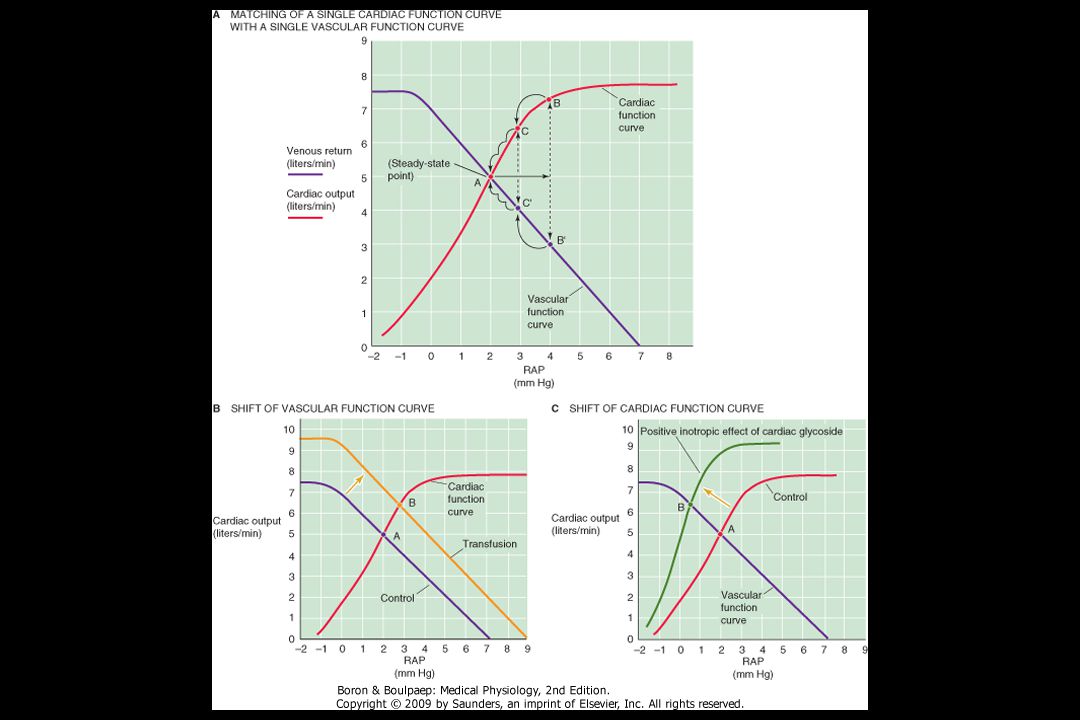
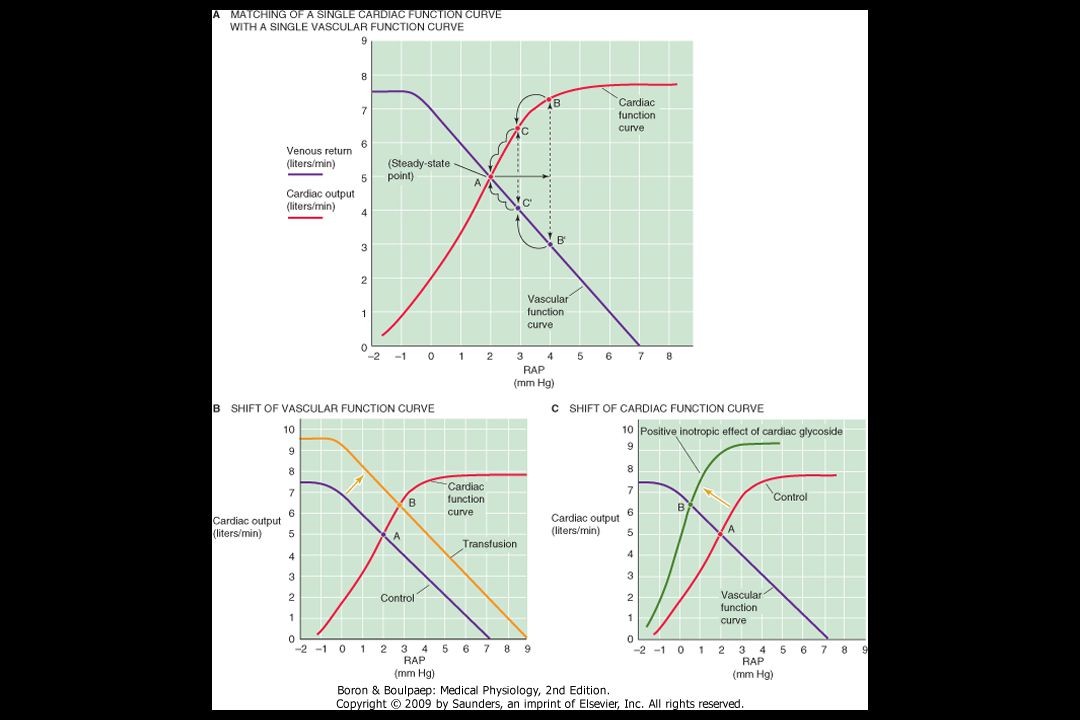
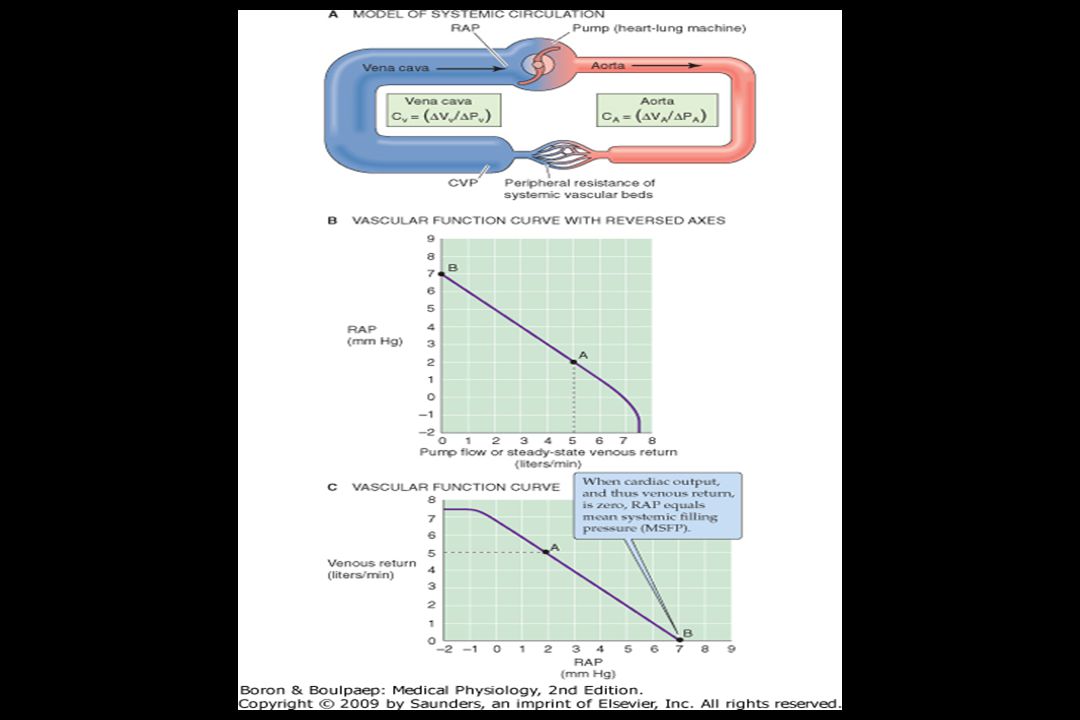
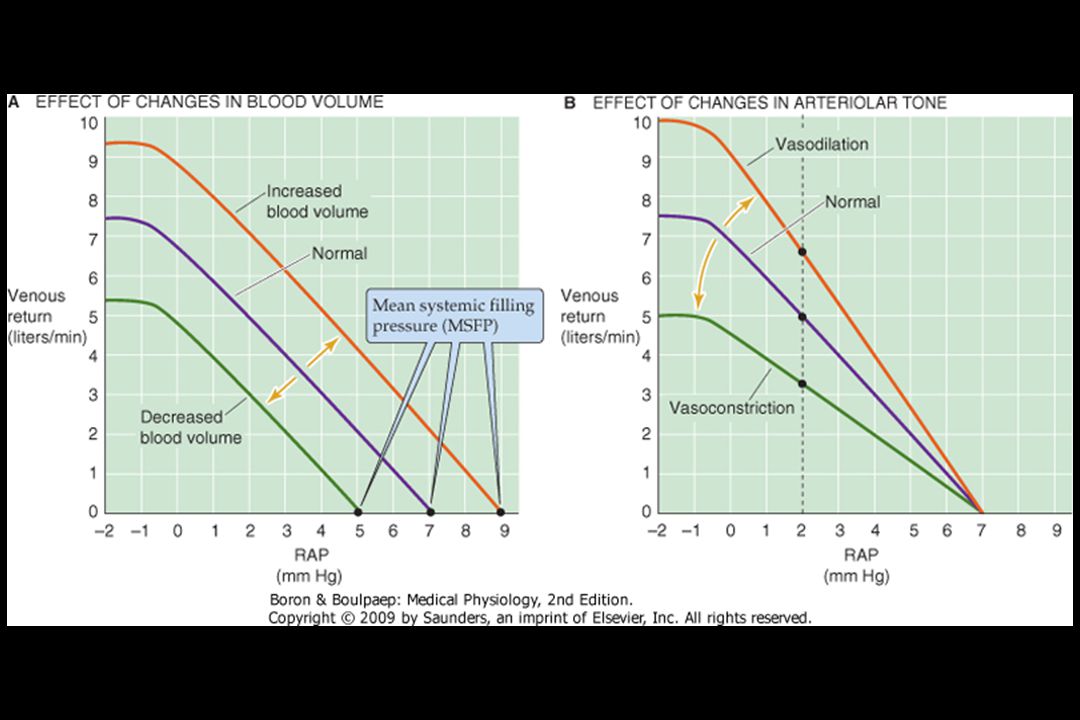
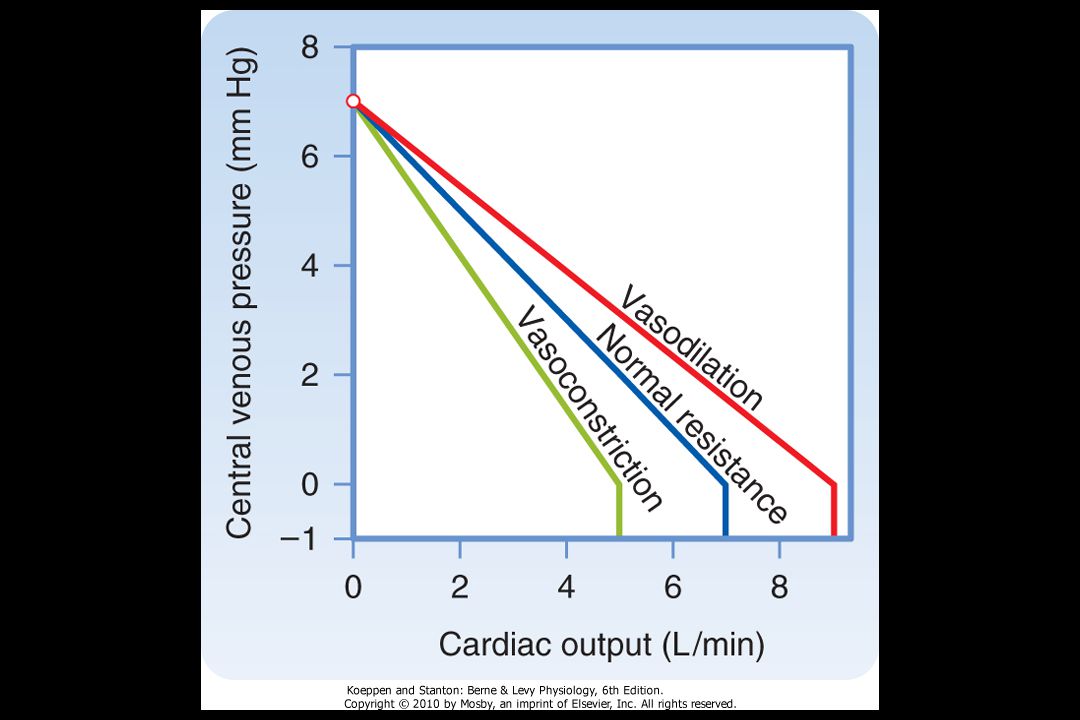
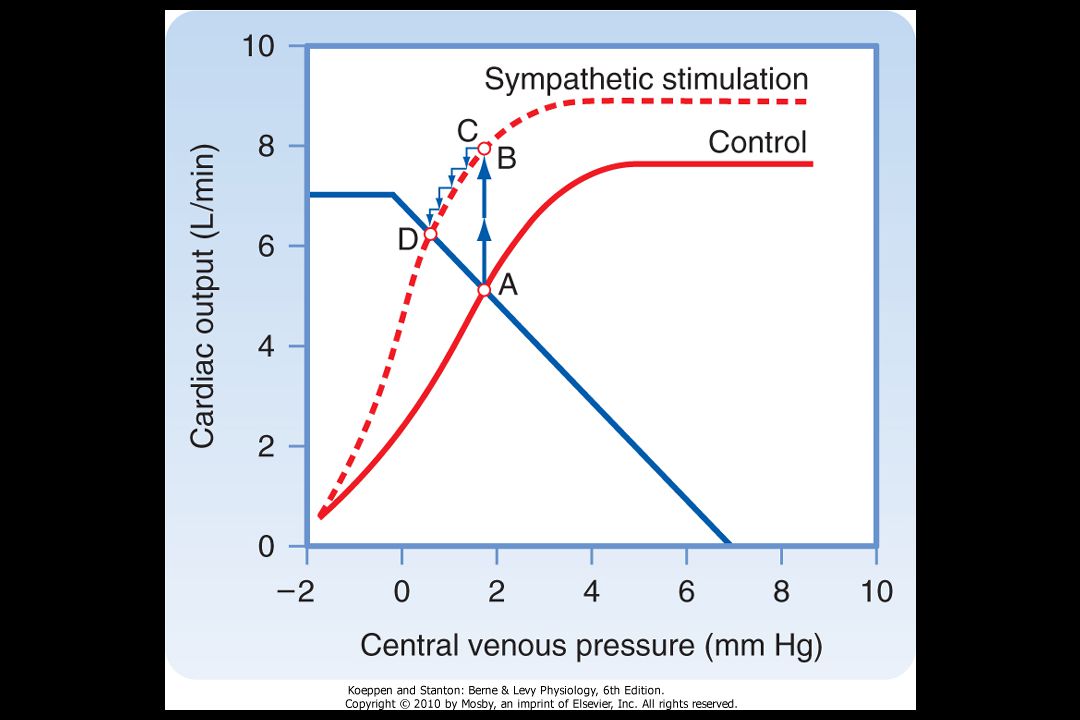
∆P = CVP - RAP CVP = central venous pressure RAP = right atrial pressure ∆P = pressure difference (i.e. driving force) for the return of blood from the periphery to the right atrium. Thus, the cardiac output steadily rises as RAP falls.
 for the return of blood from the periphery. to the right atrium. Thus, the cardiac output steadily rises as. RAP falls.")
21
Change in the venomotor tone, by constriction or dilatation of only veins, is equivalent to change
in the blood volume. Because most of the blood volume is in the veins, a pure increase in venomotor tone would be equivalent to a blood transfusion.

22
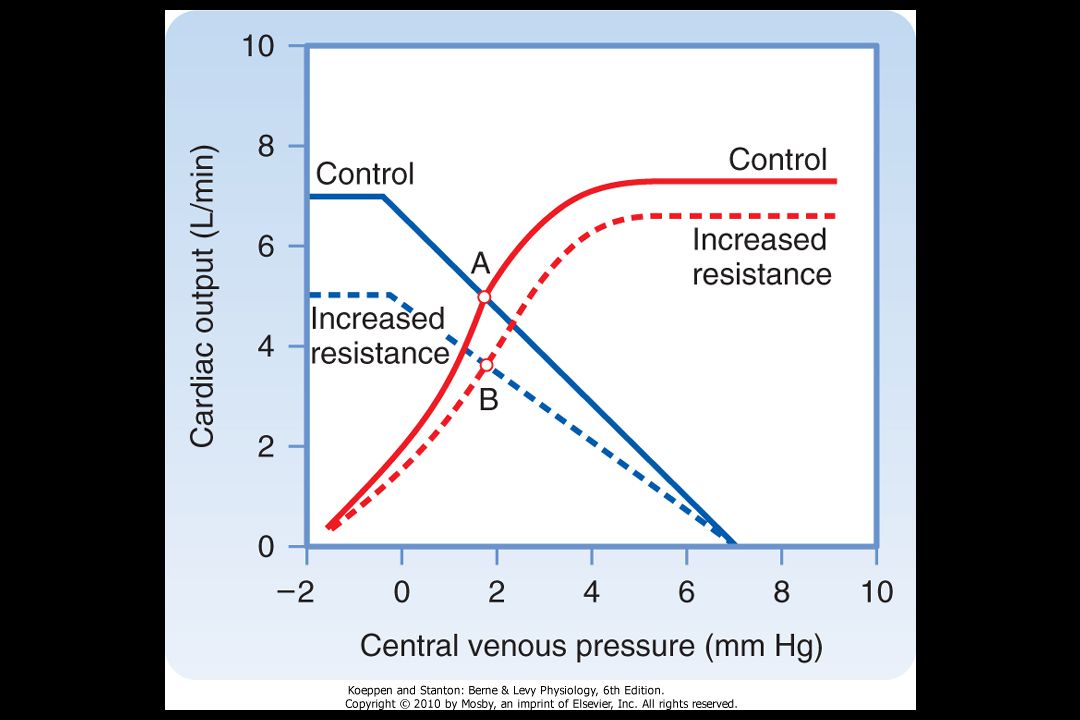
Because arterioles contain only minor fraction of the blood volume, changes in the arteriolar tone
have only little effect on MSFP and thus on the x-intercept. However, changes in the arteriolar tone can have a marked effect on the CVP

23
Normal situation ∆P = CVP – RAP = 6 mmHg – 2 mmHg = 4 mmHg venous return 5 L/min (1.25 L/1 mmHg)
Vasodilatation ∆P = CVP – RAP = 8 mmHg - 2 mmHg = 6 mmHg venous return 7.5 L/min (6 x 1.25)
")
24
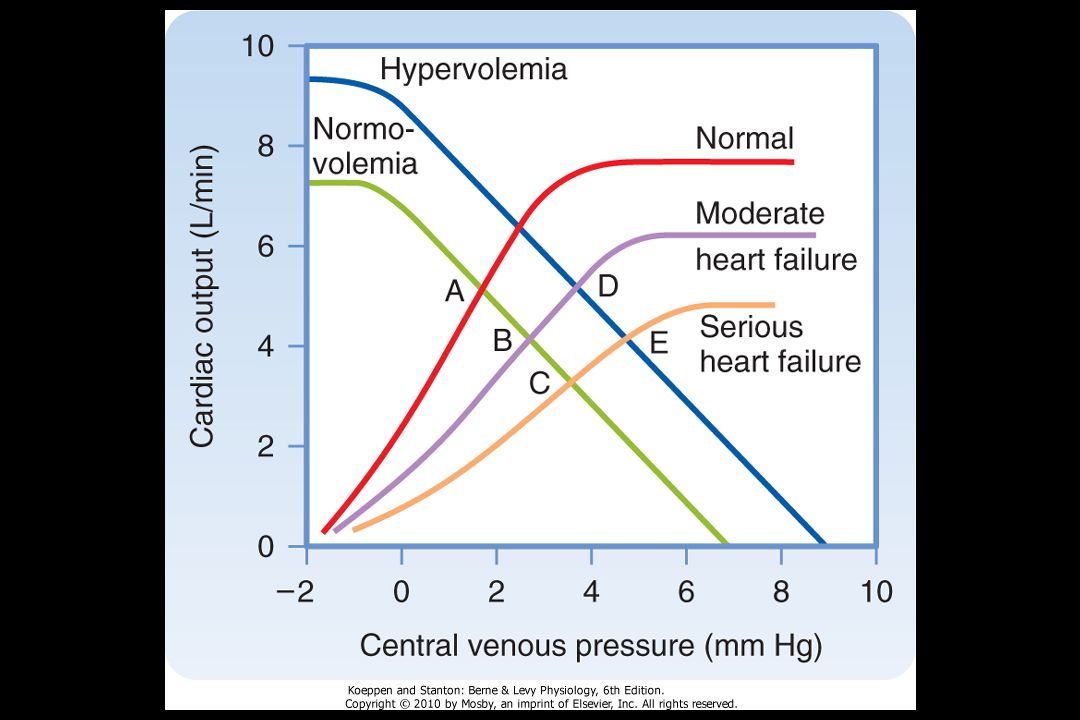
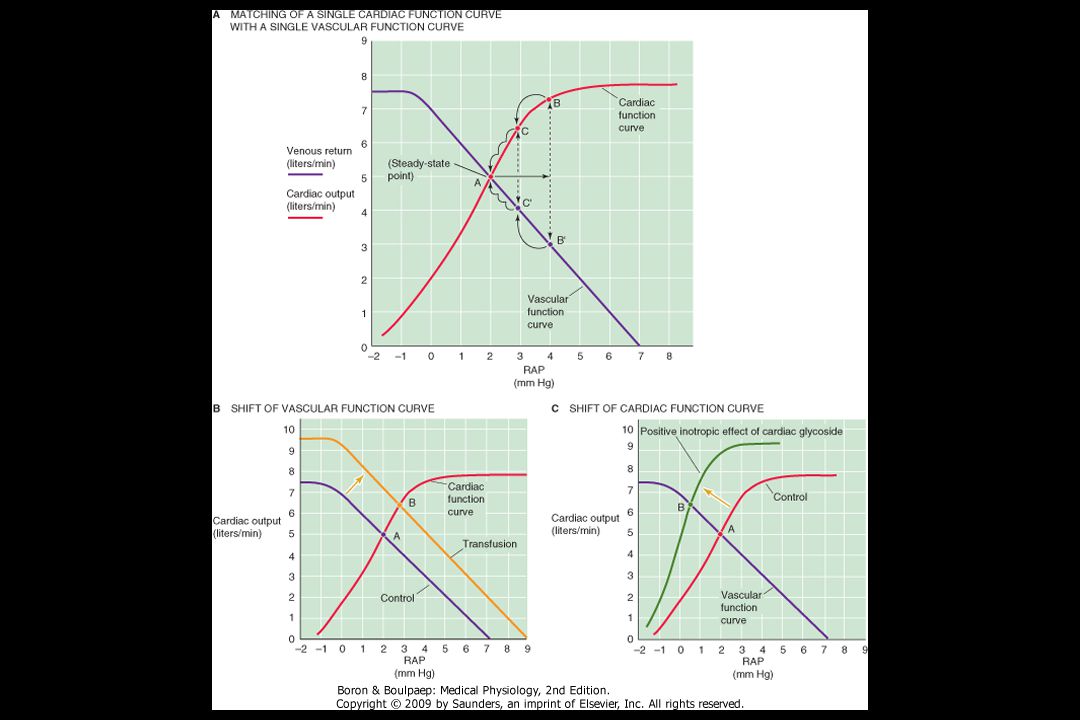
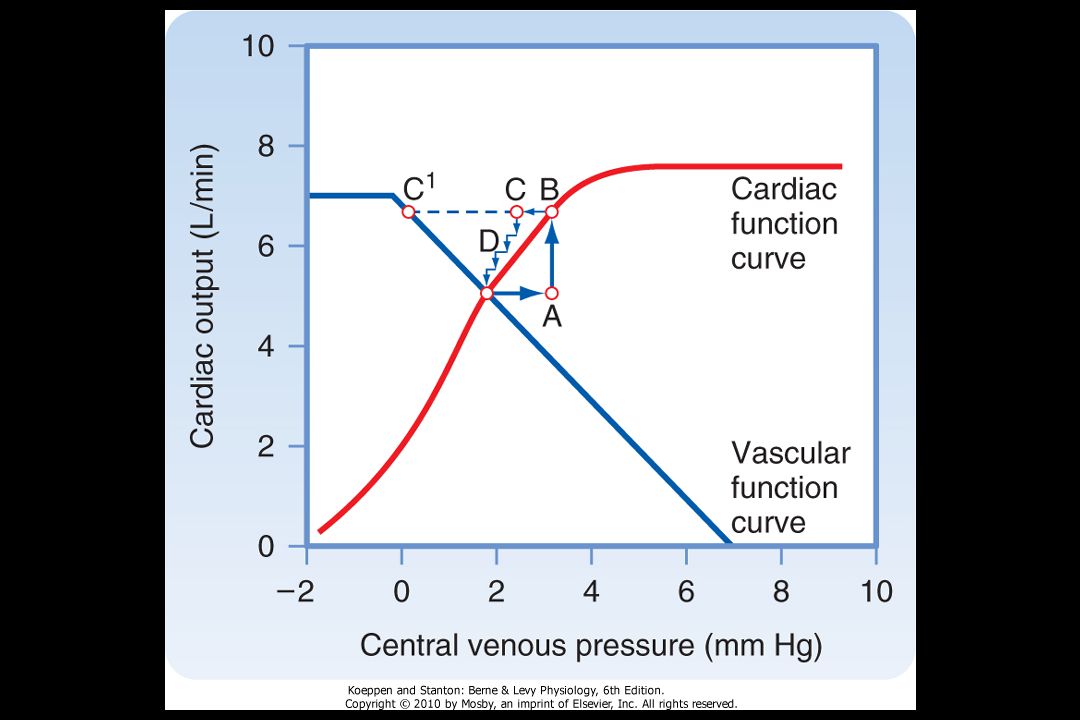
∆P = CVP - RAP Cardiac output: By sucking the right atrium dry,
it will tend to lower RAP. By pumping blood out of the heart towards the veins, it will increase CVP. Thus, the only way to produce a permanent change in cardiac output, venous return and RAP is to change at least one of the two function curve

27
Akutní mechanizmy regulace krevního tlaku
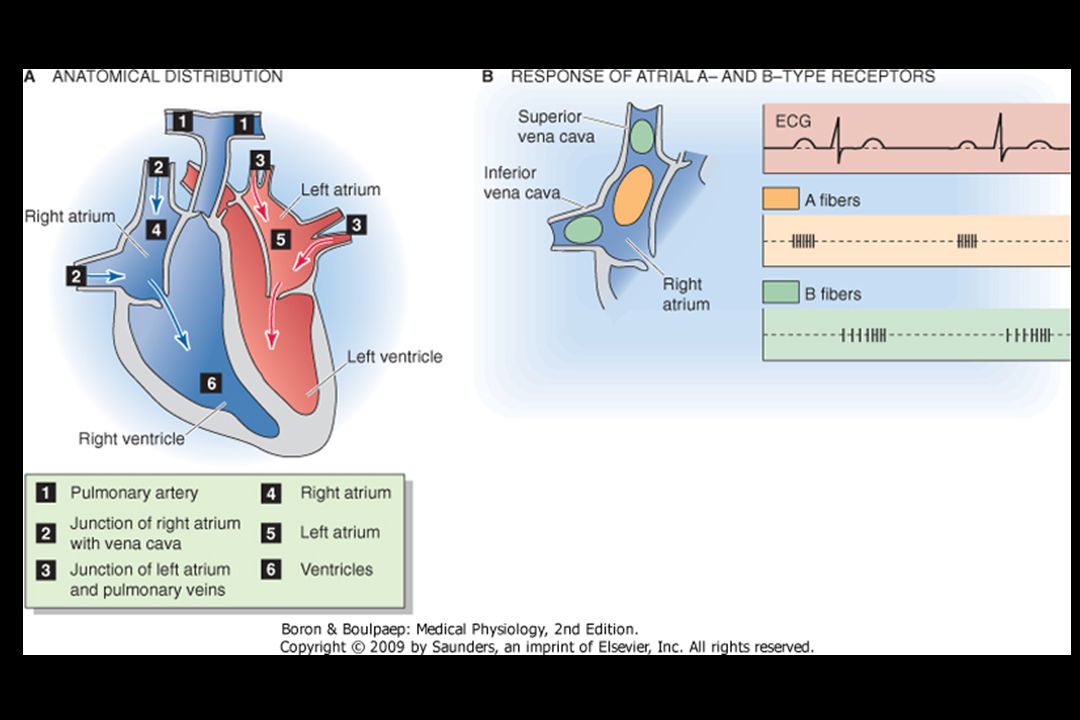
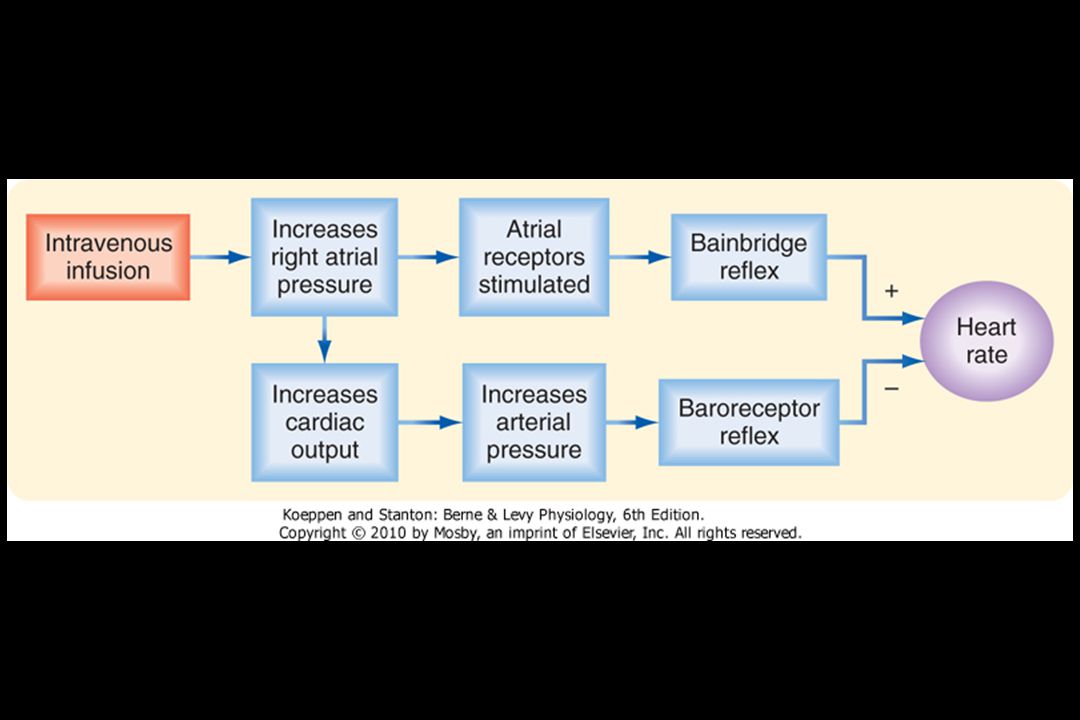
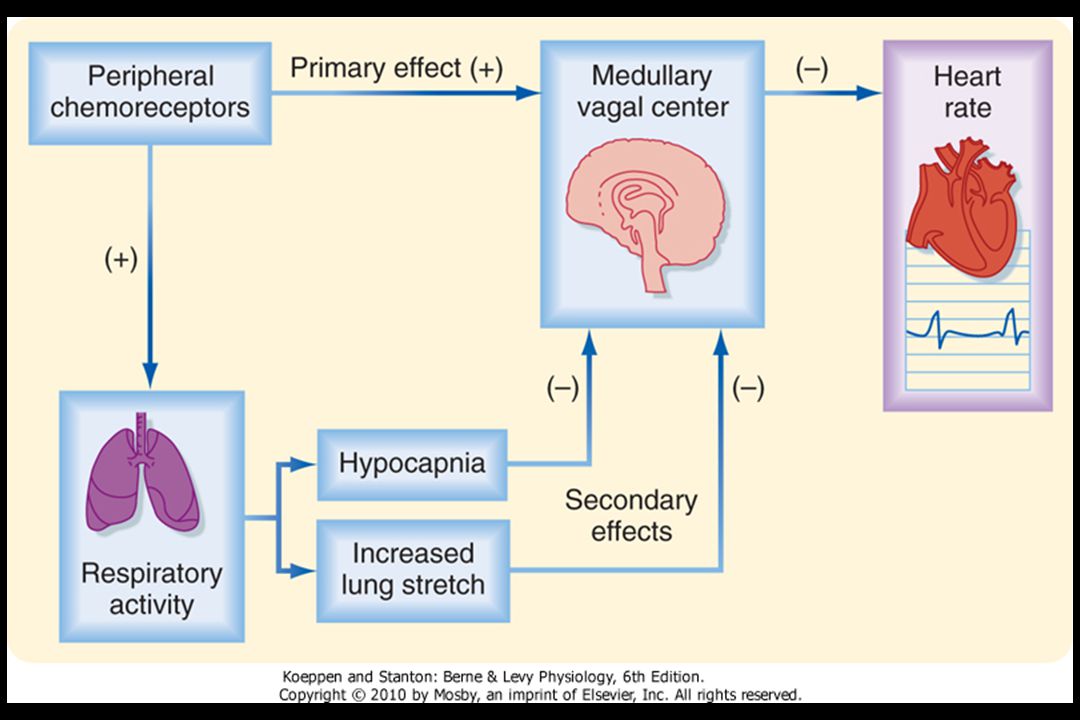
1. Arteriální baroreflex 2. Arteriální chemoreceptory 3. Bainbridgeův reflex 4. Ischemické receptory CNS

30
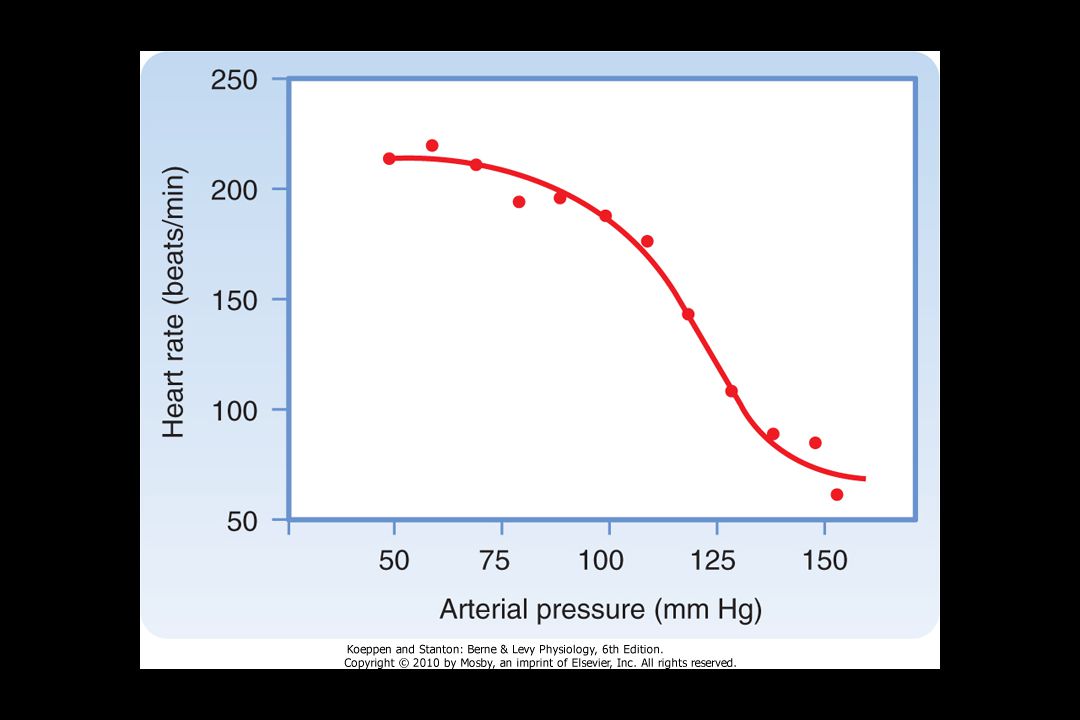
Střední arteriální tlak (mmHg)
Normální Procenta výskytu Denervovaný Střední arteriální tlak (mmHg)
")
31
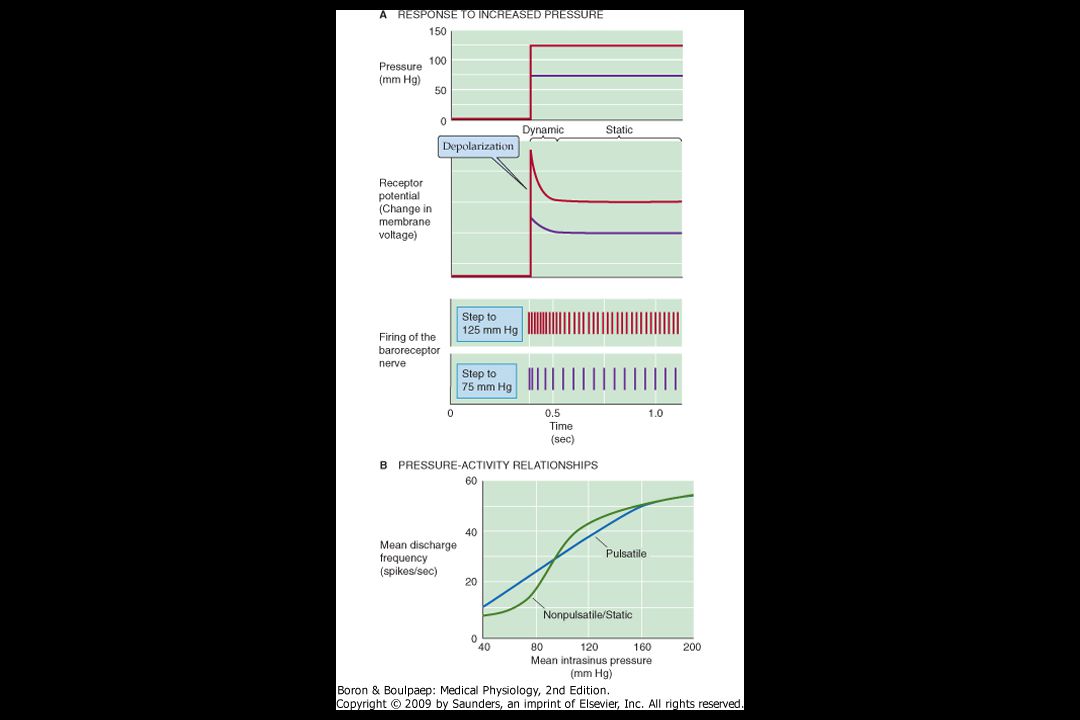
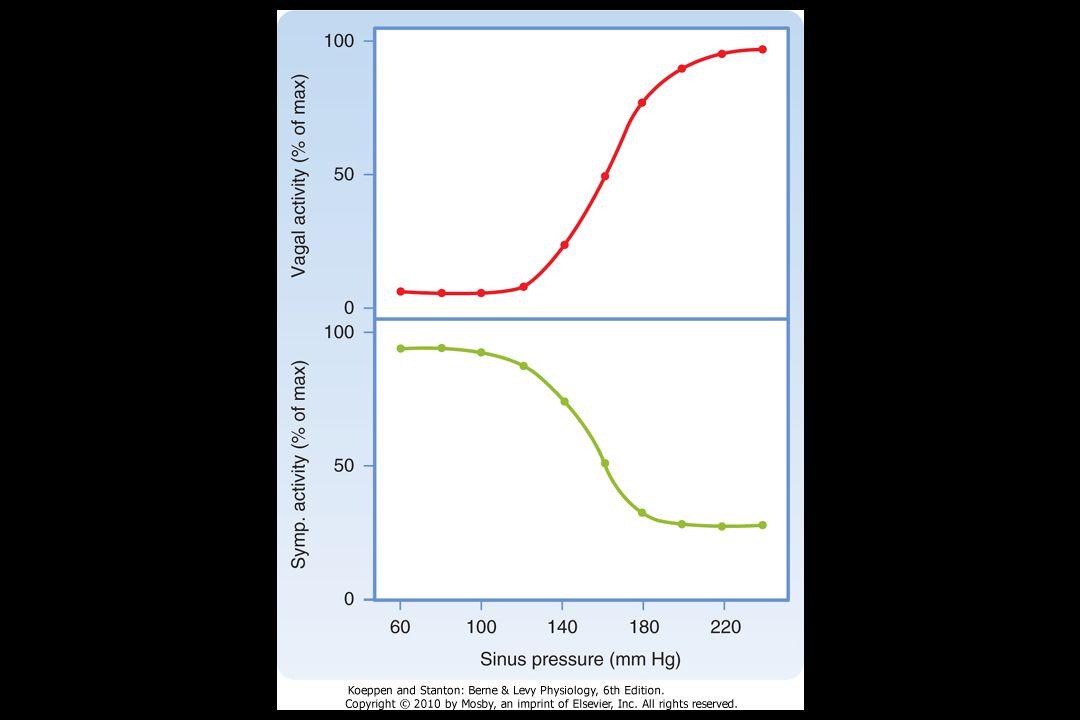
Arteriální tlak (mmHg)
„Normální“ I „Znovu nastavený“ Počet impulzů (impulz/sek) P 100 Arteriální tlak (mmHg)
 P Arteriální tlak (mmHg)")
32
Akutní mechanizmy regulace krevního tlaku
1. Arteriální baroreflex 2. Arteriální chemoreceptory 3. Bainbridgeův reflex 4. Ischemické receptory CNS

34
Akutní mechanizmy regulace krevního tlaku
1. Arteriální baroreflex 2. Arteriální chemoreceptory 3. Bainbridgeův reflex 4. Ischemické receptory CNS

37
The lecturer´s second slide was met with a more
“The first slide of the lecturer, who was an intrepid young cardiovascular physiologist, was Figure 1 from Guyton and Coleman´s epic paper. It was clear that the audience was already becoming nervous. There was some whispering, shuffling, and a sense of unease. The lecturer´s second slide was met with a more definite response. There was derision, laughter, and spontaneous comments from the audience….. I witnessed, for the only time in my academic life, a lecturer being chased from the podium by the audience” Christopher S. Wilcox

40
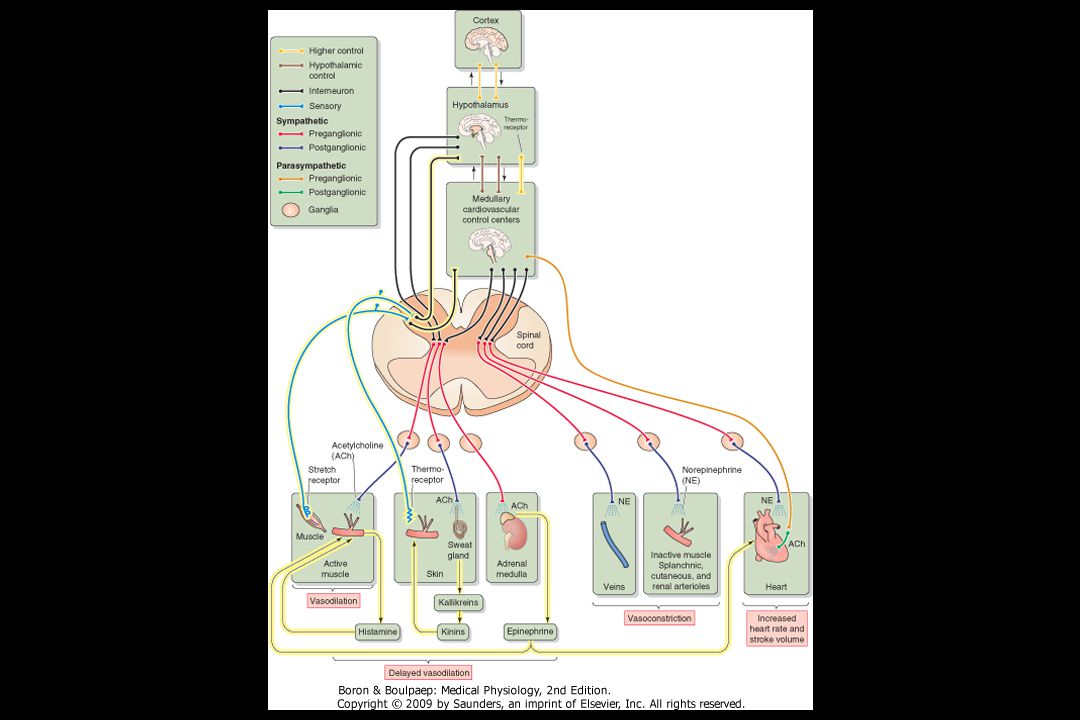
Vazodilatace Vazokonstrikce

42
Amount Amount Amount % of Filtered
Filtration, Reabsorption and Excretion Rates of Different Substances by the Kidneys Amount Amount Amount % of Filtered Filtered Reabsorbed Excreted Load Reabsorbed Glucose (g/day) Bicarbonate (mmol/day) Sodium Chloride Potassium Creatinine
 Bicarbonate (mmol/day) Sodium Chloride Potassium Creatinine")
44
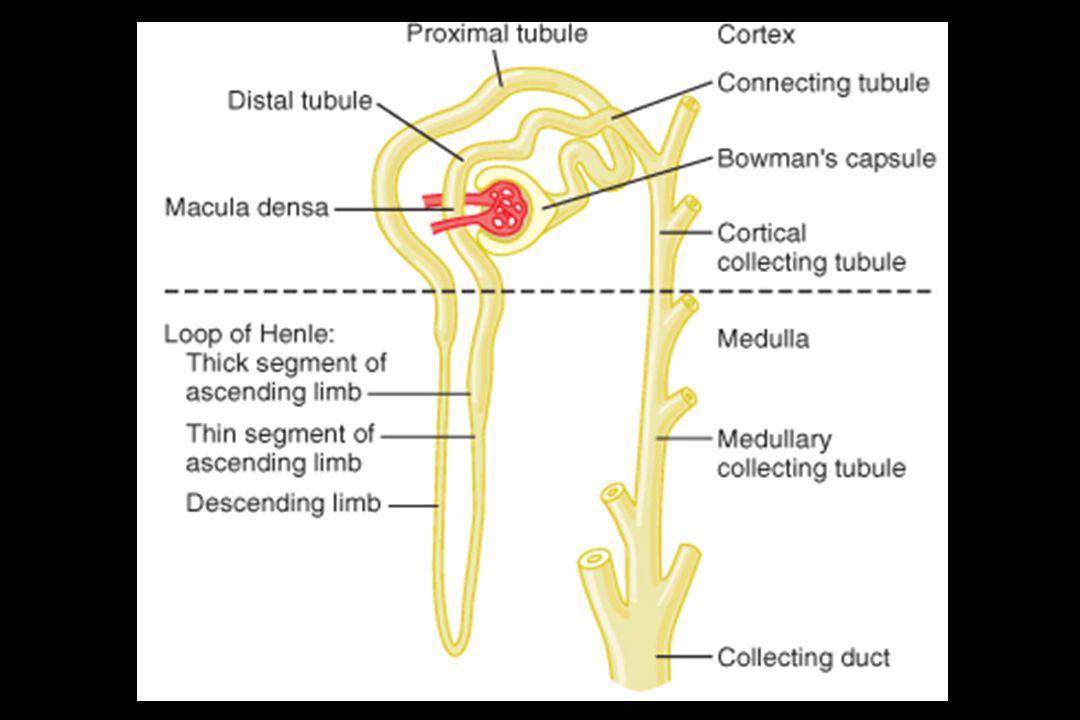
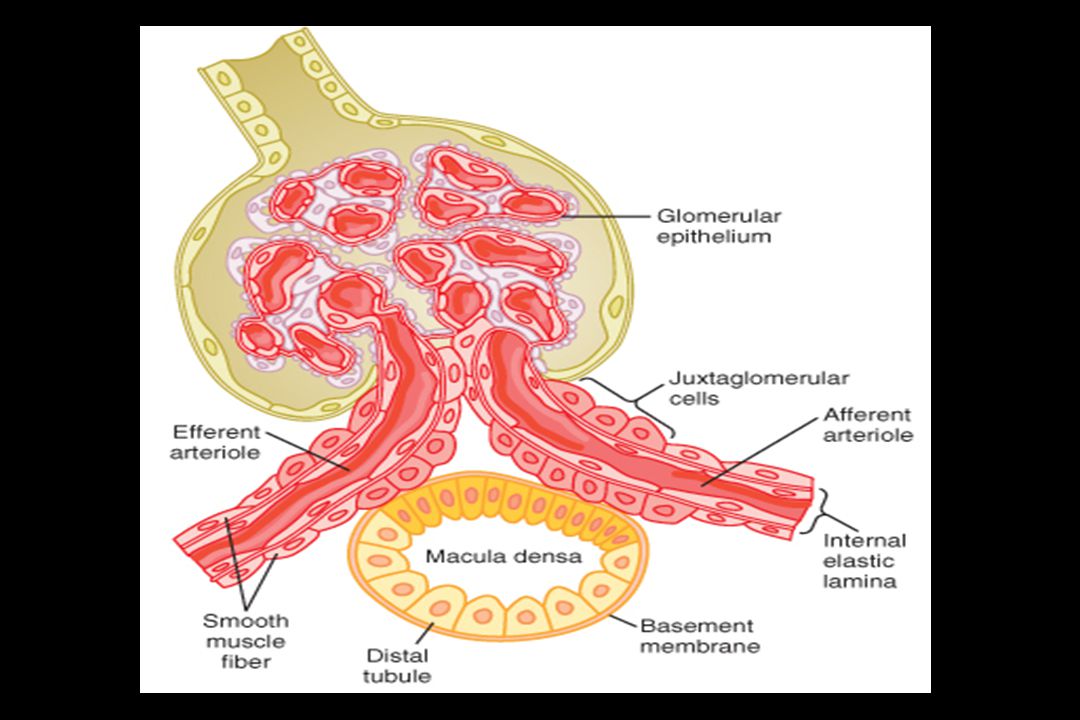
Tubuloglomerular Feedback
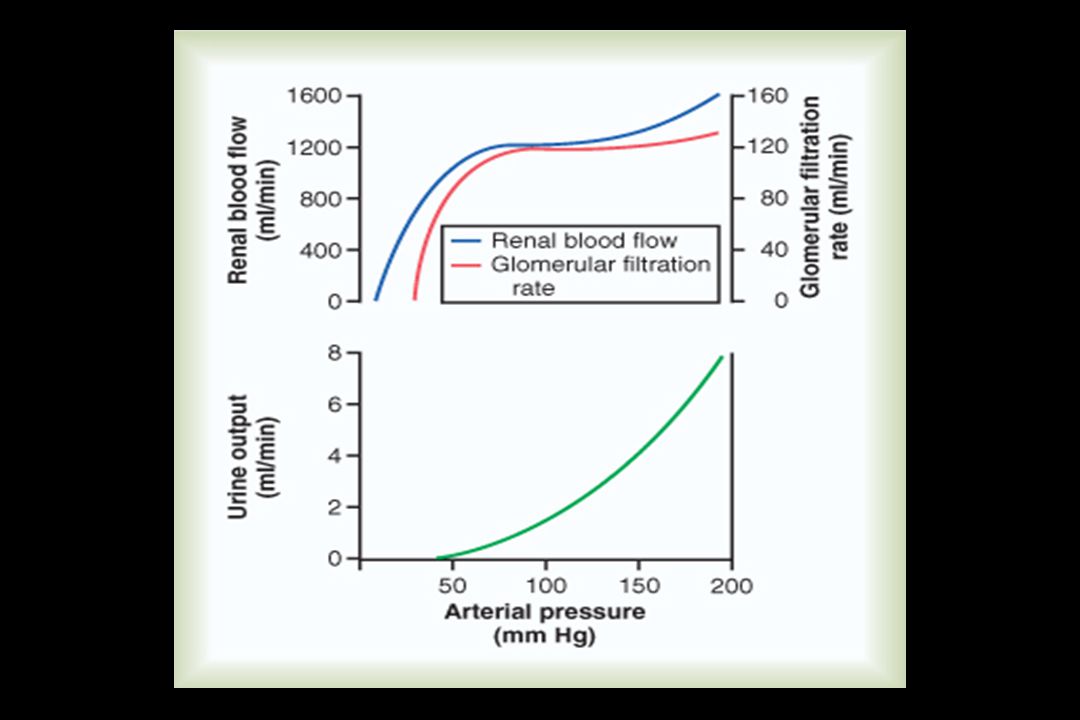
Autoregulation of Glomerular Filtration Rate and Renal Blood Flow Myogenic Mechanism Tubuloglomerular Feedback

48
Příjem nebo vylučování sodíku
(x normálu) Equilibrium Renálně perfuzní tlak (mmHg)
 Equilibrium. Renálně perfuzní tlak (mmHg)")
49
Příjem nebo vylučování sodíku
Equilibrium B Příjem nebo vylučování sodíku (x normálu) Equilibrium A Renálně perfuzní tlak (mmHg)
 Equilibrium A. Renálně perfuzní tlak (mmHg)")
50
Příjem nebo vylučování sodíku
A B Příjem nebo vylučování sodíku (x normálu) Equilibrium Renálně perfuzní tlak (mmHg)
 Equilibrium. Renálně perfuzní tlak (mmHg)")
51
Příjem nebo vylučování sodíku
(x normálu) Equilibrium A Equilibrium B Renálně perfuzní tlak (mmHg)
 Equilibrium A. Equilibrium B. Renálně perfuzní tlak (mmHg)")
52
Příjem nebo vylučování sodíku
(x normálu) C A B Renálně perfuzní tlak (mmHg)
 C. A. B. Renálně perfuzní tlak (mmHg)")
53
Formy Hypertenze A. Esentiální (Primární) Hypertenze
B. Sekundární Hypertenze 1. Renovaskulární Hypertenze 2. Renální (parenchymatózní) Hypertenze 3. Endokrinně Podmíněné Formy Hypertenze a/ Primární hyperaldosteronismus b/ Pseudohyperaldosterinismus - Liddleuv syndrom c/ Pseudohyperaldosterinismus - způsobený defektem 11-ßHSD d/ Hyperaldosterinismus ovlivnitelný glukokortikoidy e/ Cushingův sysndrom f/ Feochromocytom
 Hypertenze. 3. Endokrinně Podmíněné Formy Hypertenze. a/ Primární hyperaldosteronismus. b/ Pseudohyperaldosterinismus - Liddleuv syndrom. c/ Pseudohyperaldosterinismus - způsobený defektem 11-ßHSD. d/ Hyperaldosterinismus ovlivnitelný glukokortikoidy. e/ Cushingův sysndrom. f/ Feochromocytom.")
54
Primární hyperaldosteronismus
Nadbytek mineralokortikoidů produkovaných adenomem (tzv. Connův syndrom) způsobí: 1. Zvýšenou aktivitu Na+-K+ pumpy v bazolaterální membráně. 2. Zvýšenou aktivitu epiteliálních kanálů pro Na+ (ENaC) v luminální membráně.
 způsobí: 1. Zvýšenou aktivitu Na+-K+ pumpy v bazolaterální membráně. 2. Zvýšenou aktivitu epiteliálních kanálů pro Na+ (ENaC) v luminální membráně.")
55
Primární hyperaldosteronismus
lumen intersticium Na+ Cl- 3Na+ 2K+ Na+ K+

56
Liddleuv syndrom - pseudohyperaldosteronismus
Tento syndrom je způsoben mutací jedné ze tří podjednotek ENaC kanálu, což způsobuje, že tento kanál zůstává konstitutivně aktivní

57
Liddleúv syndrom - pseudohyperaldosterinismus
lumen intersticium Na+

58
Pseudohyperaldosteronismus
způsobený defektem 11-beta-hydroxysteroiddehydrogenázy Mineralokortikoidní receptor je nitrobuněčný cytoplazmatický protein, který může vázat jak aldosteron, tak i glukokortikoidní hormon kortizol. Buňky (distálního tubulu) mají na svém povrchu enzym 11-ß-HSD, která mění kortizol na kortizon, což sekundárně způsobí, že v okolí těchto buněk je lokálně dostupný pouze aldostern
 mají na svém povrchu. enzym 11-ß-HSD, která mění kortizol na kortizon, což sekundárně. způsobí, že v okolí těchto buněk je lokálně dostupný pouze aldostern.")
59
lumen intersticium Na+ Cl- 3Na+ 2K+ Na+ K+

60
Pseudohyperaldosteronismus
příznivě ovlivnitelný glukokortikoidy Dochází k nadprodukci aldosteronu a gen aldosteronsyntáza je napojen na regulační gen 11-betahydroxylázy, což dostává syntézu pod kontrolu ACTH.

61
Hyperaldosterinismus – ovlivněný glukokortikoidy
lumen intersticium Na+ Cl- 3Na+ 2K+ Na+ K+

62
Cushingův syndrom V případě nadměrného (farmakologického) podávání glukokortikodiů, tak i funkční 11-ß-HSD není schopna „odbourat“ všechen kortizol a dochází k aktivaci mineralokortikoidních receptorů

63
Cushingův syndrom lumen intersticium ALDO N GR Na+

64
Feochromocytom Nádor dřeně nadledvin produkuje enormní množství katecholaminů

65
Děkuji za pozornost

66
Tady toho necháme

78
Síla zpětnovazebního mechanizmu
8 8 !! 11 10 9 8 7 6 5 4 3 2 1 - Ischemické reakce CNS Tlakově-natriuretický mechanizmus ledvin Baroreceptory Iniciální akutní změna TK Síla zpětnovazebního mechanizmu Chemoreceptory Aldosteron Relaxace arterií Přesun tekutiny RAS z plazmy 8 Sekundy Minuty Hodiny Dny Čas po náhlé změně TK 78

83
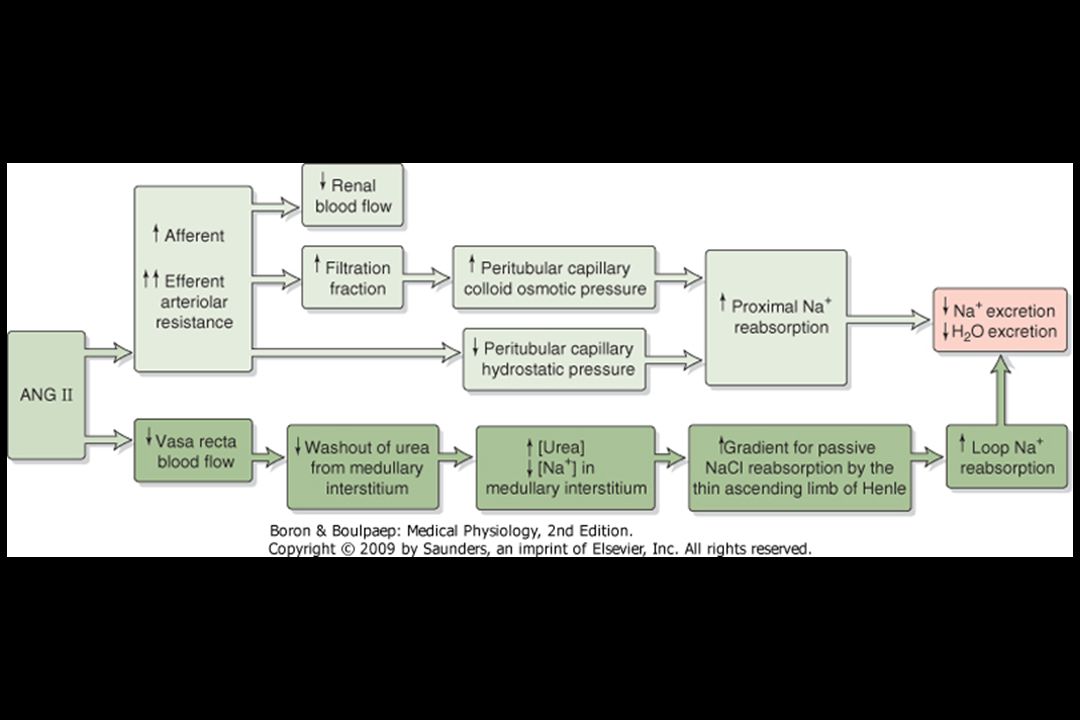
AT1A B2 Kininogen Angiotensinogen Kallikrein Renin Kinins
Angiotensin I ACE Angiotensin II AT1A AT1B AT2 B1 B2

86
ANGIOTENZINOGEN Renin ANGIOTENZIN I ACE ANGIOTENZIN II Kůra nadledvin Ledviny Střevo CNS Perif. nerv. systém Hladká sval. cév Srdce Vazokonstr. Transport Aldo. Reabsorbce Na v distálním tubulu Výdej Vazopresinu Žízeň Celková perif. rezistence Srdeční Výdej Zachování OECT

90
Percent of filtered load reabsorbed (%)
Comparison of sodium and water reabsorption along the tubule Percent of filtered load reabsorbed (%) Tubular segment Sodium Water Proximal tubule Descending thin limb of Henle´s loop Ascending thin limb and thick ascending limb of Henle´s loop Distal convoluted tubule Collecting-duct system (during water-loading) >24 (during dehydration)
 Tubular segment Sodium Water. Proximal tubule Descending thin limb of Henle´s loop Ascending thin limb and thick ascending limb of Henle´s loop. Distal convoluted tubule 5 0. Collecting-duct system (during water-loading) >24 (during dehydration)")
91
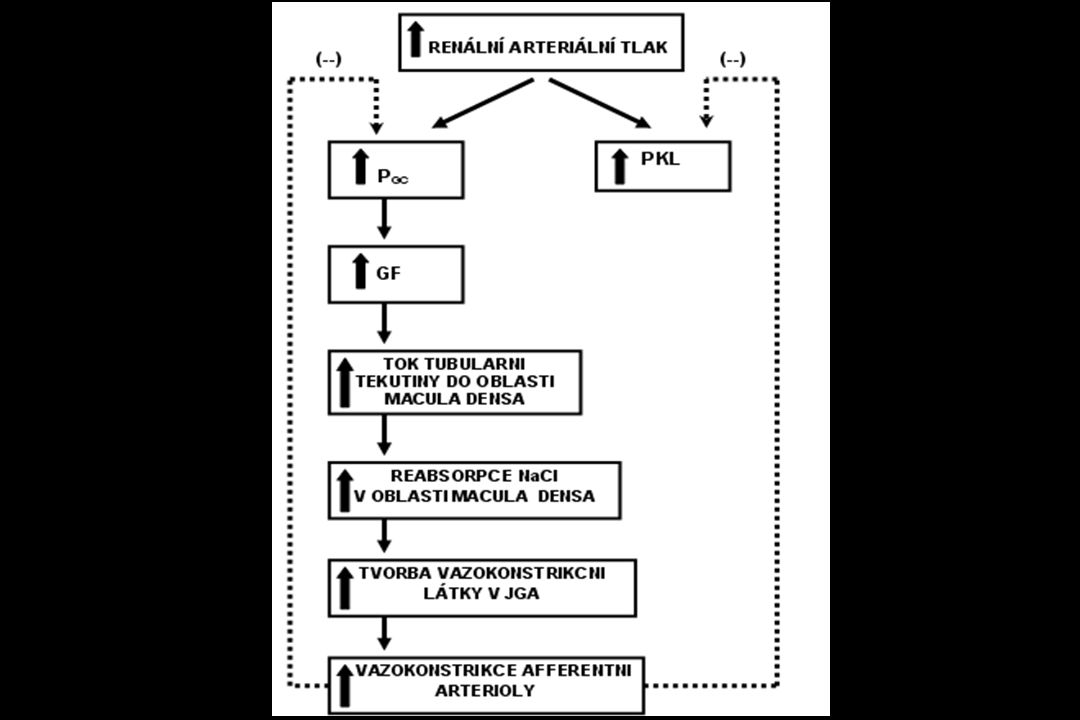
- - + ARTERIÁLNÍ KREVNÍ TLAK Příjem soli v potravě
Nepozorovatelné ztráty (kůží, plícemi, stolicí) Vylučování sodíku do moče - - + RAS KKS ANF NO Endothelin Vasopressin Katecholamíny Prostaglandíny Čistá sodíková rovnováha Krevní objem OECT ARTERIÁLNÍ KREVNÍ TLAK Periferní cévní rezistence Srdeční frekvence a srdeční kontraktilita Střední cirkulační tlak Žilní návrat Srdeční výdej
 Vylučování sodíku do moče RAS KKS ANF NO Endothelin Vasopressin Katecholamíny Prostaglandíny. Čistá sodíková rovnováha. Krevní objem. OECT. ARTERIÁLNÍ KREVNÍ TLAK. Periferní cévní rezistence. Srdeční frekvence a srdeční kontraktilita. Střední cirkulační tlak. Žilní návrat. Srdeční výdej.")
92
ARTERIÁLNÍ KREVNÍ TLAK
Počáteční vzestup PCR Počáteční vzestup OECT Nervové nebo hormonální podněty OECT Vazokonstrikční účinky Retence sodíku a vody v ledvinách Efektivní krevní objem Srdeční výdej Kapacita cévního řečiště Perfůze tkání Autoregulační úprava rezistence Vzestup PCR ARTERIÁLNÍ KREVNÍ TLAK

96
96

97
97

98
98

99
99

100
100

101
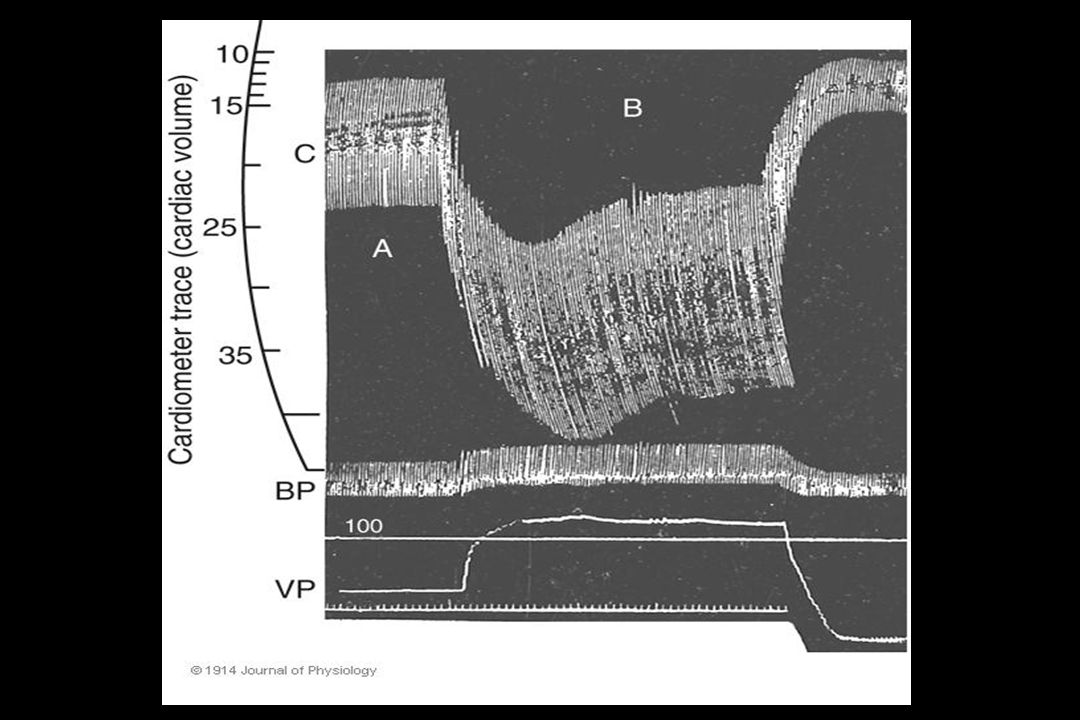
Starling’s experiment
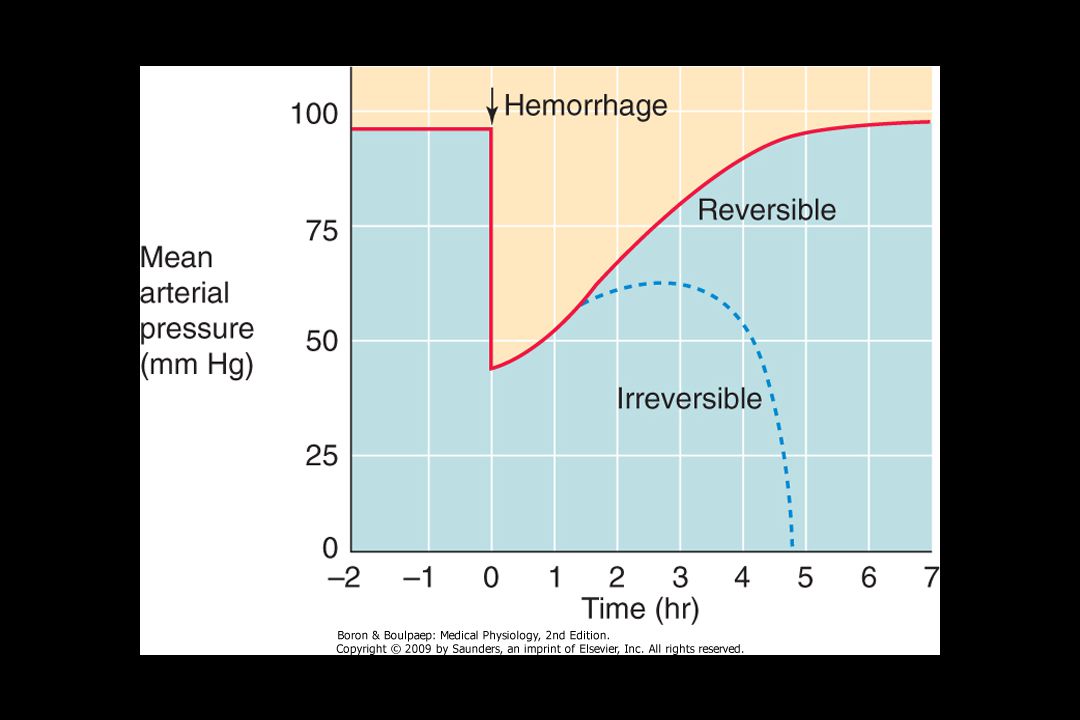
Arterial pressure or ‘afterload’ Central venous pressure or ‘filling pressure’ or ‘preload’ ; Following studies on contracting frog hearts by Otto Frank, Starling & colleagues set up an isolated canine heart–lung preparation, in which they could control the pressure of venous blood filling the ventricles (‘central venous pressure’, ‘filling pressure’ or ‘preload’ (an inaccurate term)). They recorded the effect of filling pressure on stroke volume using a glass bell cardiometer, which wrote on a rotating smoked drum. Arterial pressure (often called, inaccurately, ‘afterload’) was also controlled. (Medical relevance: in patients the filling pressure falls after a haemorrhage, and can be raised by an intravenous infusion of saline or blood.) Stroke vol. 101 Hodder Arnold / An Introduction to Cardiovascular Physiology © 2010 J. Rodney Levick 101
). They recorded the effect of filling pressure on stroke volume using a glass bell cardiometer, which wrote on a rotating smoked drum. Arterial pressure (often called, inaccurately, ‘afterload’) was also controlled. (Medical relevance: in patients the filling pressure falls after a haemorrhage, and can be raised by an intravenous infusion of saline or blood.) Stroke vol Hodder Arnold / An Introduction to Cardiovascular Physiology © 2010 J. Rodney Levick")
112
TK = SV x PCR TK = arteriální krevní tlak SV = srdeční výdej
(Tepový objem x Srdeční frekvence) TK = arteriální krevní tlak SV = srdeční výdej PCR = periferní cévní rezistence
 TK = arteriální krevní tlak. SV = srdeční výdej. PCR = periferní cévní rezistence.")
Podobné prezentace
























 vylučované kůrou nadledvinek (aldosteron, kortisol); 2) vylučované pohlavními žlázami (progesteron, testosteron, estradiol)>")





>")