Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Nespecifické střevní záněty
Jarmila Vospělová

2
Nespecifické střevní záněty (NSZ)
idiopatická chronická onemocnění (IBD – inflammatory bowel disease) Crohnova nemoc (CD) ulcerózní kolitida (UC) etiologie nejasná přirozený průběh charakterizován obdobím remisí a nepředvídatelných exacerbací IBD - a group of idiophatic, chronic disoders includes Crohn disease and ulcerative colitis. The etiology is poorly understood and the natural course is characterised by unpredictable exacerbations and remissions
 Crohnova nemoc (CD) ulcerózní kolitida (UC) etiologie nejasná. přirozený průběh charakterizován obdobím remisí a nepředvídatelných exacerbací. IBD - a group of idiophatic, chronic disoders includes Crohn disease and ulcerative colitis. The etiology is poorly understood and the natural course is characterised by unpredictable exacerbations and remissions.")
3
Nespecifické střevní záněty (NSZ)
u 1/3 pacientů začíná onemocnění v adolescenci a čásné dospělosti (15-25let věku) NSZ může začít v kterémkoliv věku The most common time of onset of IBD is during adolescents and young adalthood. Nonetheless, IBD may begin in the 1st yr of life. IBD is more common in urban areas than in rural areas. In developed countries, these disoders are the major causes of chronic intestinal inflammation in children. This picture shows the age distribution in one group of patients with IBD before 18 yr of life.
 NSZ může začít v kterémkoliv věku. The most common time of onset of IBD is during adolescents and young adalthood. Nonetheless, IBD may begin in the 1st yr of life. IBD is more common in urban areas than in rural areas. In developed countries, these disoders are the major causes of chronic intestinal inflammation in children. This picture shows the age distribution in one group of patients with IBD before 18 yr of life.")
4
NSZ - epidemiologie prevalence severojižní gradient UC 150/ CD / incidence (2,5-6)/ ve věku 0-20let - incidence UC zůstává konstantní - incidence CD se zvyšuje v posledních 10 letech The prevalence is frequency of individuals with a certain disease at a certain point in time, expressed in cases per persons in the general population. The incidence od IBD in children and adolescents is about 5 new cases per persons under 18 years of age The incidence is the yearly rate of newly diagnosed disease per persons.
/ ve věku 0-20let - incidence UC zůstává konstantní - incidence CD se zvyšuje v posledních 10 letech. The prevalence is frequency of individuals with a certain disease at a certain point in time, expressed in cases per persons in the general population. The incidence od IBD in children and adolescents is about 5 new cases per persons under 18 years of age. The incidence is the yearly rate of newly diagnosed disease per persons.")
5
Patogeneze NSZ genetika - riziko NSZ v rodinách postiženého pacienta % - oba rodiče s NSZ – riziko NSZ pro dítě 35% vlivy prostředí - cigaretový kouř - skladba jídelníčku - infekce (mycobacteria) Both genetic and environmental influences are involved in the pathogenesis of IBD. The risk of IBD in family members of an affected individual has been reported in the range of 7-22%. A child whose parents both have IBD has a greater than 35% chance of acquiring the disorder. Relatives of an individual with UC have a greater risk of acquiring UC than CD. Relatives of an individual with CD have a greater risk of acquiring this disorder. The two diseases may occur in the same family. Within the family CD may develop at an earlier age among the 2nd generation. Cigarette smoking is a risk factor for CD but paradoxically protects against UC.
 Both genetic and environmental influences are involved in the pathogenesis of IBD. The risk of IBD in family members of an affected individual has been reported in the range of 7-22%. A child whose parents both have IBD has a greater than 35% chance of acquiring the disorder. Relatives of an individual with UC have a greater risk of acquiring UC than CD. Relatives of an individual with CD have a greater risk of acquiring this disorder. The two diseases may occur in the same family. Within the family CD may develop at an earlier age among the 2nd generation. Cigarette smoking is a risk factor for CD but paradoxically protects against UC.")
6
děti s NSZ mezi dětmi s CAP (pod 1%)
Příznaky NSZ chronická bolest břicha (CAP) jeden z hlavních příznaků pacientů s NSZ CAP postihuje 10-15% jinak zdravých dětí a adolescentů děti s NSZ mezi dětmi s CAP (pod 1%)
 jeden z hlavních příznaků pacientů s NSZ. CAP postihuje 10-15% jinak zdravých dětí a adolescentů. děti s NSZ mezi dětmi s CAP (pod 1%)")
7
Srovnání klinických příznaků u CD a UC

8
Příznaky NSZ CD - příznaky se objevují pomalu a mohou být nespecifické (bledost, změny nálad, neprospívání, hmotnostní úbytek) - diagnóza je stanovena pozdě (diagnostická latence 12 měsíců) UC – rozhodující příznak stolice s krví (90% pacientů) - diagnóza je stanovena mnohem dříve (diagnostická latence 6 měsíců) CD often develops slowly with unspecific symptoms (pallor, mood swings, failure to thrive, weight loss). This is one of the reasons that the diagnosis is established very late, particularly in patients under 10 years of age. Average diagnostic latency is 12 month (range 1 month to 7 years). This period (means before ten years of age) is characterised of rapid physical development in children, and such latency in diagnosis may have negative irreversible effects. The leading symptom in UC is bloody diarrhea, occuring in over 90% of patients. The diagnosis is made much earlier than in CD. Diagnostic latency is in average 6 months.
 - diagnóza je stanovena pozdě (diagnostická latence 12 měsíců) UC – rozhodující příznak stolice s krví (90% pacientů) - diagnóza je stanovena mnohem dříve (diagnostická latence 6 měsíců) CD often develops slowly with unspecific symptoms (pallor, mood swings, failure to thrive, weight loss). This is one of the reasons that the diagnosis is established very late, particularly in patients under 10 years of age. Average diagnostic latency is 12 month (range 1 month to 7 years). This period (means before ten years of age) is characterised of rapid physical development in children, and such latency in diagnosis may have negative irreversible effects. The leading symptom in UC is bloody diarrhea, occuring in over 90% of patients. The diagnosis is made much earlier than in CD. Diagnostic latency is in average 6 months.")
9
Extraintestinální manifestace u dětí s NSZ v době diagnózy

10
Opoždění růstu často 1.příznak CD u dětí
může předcházet rozvoj dalších příznaků CD až o několik let často není detekováno včas rozpoznání snadné!!! (antropometrické parametry, percentilové grafy výšky, váhy, BMI) je ireverzibilní pokud není včas rozpoznáno a léčeno
 je ireverzibilní pokud není včas rozpoznáno a léčeno.")
11
Antropometrické parametry – výška/věk

12
Růstová rychlost

13
Antropometrické parametry – hmotnost/věk

14
Opoždění růstu percentilový pokles (velká odchylka od předešlého percentilu - patologické) pokles pod třetí percentil (patologické) predikce cílové výšky dle výšky rodičů (průměr součtu výšky otce a matky v centimetrech + 6,5 pro chlapce a - 6,5 pro dívky) růstová rychlost 1x/rok (patologická pokud klesne o víc jak 25 percentilů, časně detekovatelný parametr)
 růstová rychlost 1x/rok (patologická pokud klesne o víc jak 25 percentilů, časně detekovatelný parametr)")
15
Extraintestinální manifestace
klouby - kolitická artritida - axiální artritida (ileosakrální), HLA B27+ kůže - erythema nodosum - pyoderma gangrenosum - aftózní stomatitida, gingivitida - psoriasa Erythema nodosum occurs most often in association with CD. pyoderma gangrenosum occurs more often in patients with UC. Other dermatological entities in patients with CD are: aphthotic stomatitis, gingivitis, cheilitis, psoriasis.
, HLA B27+ kůže - erythema nodosum - pyoderma gangrenosum - aftózní stomatitida, gingivitida - psoriasa. Erythema nodosum occurs most often in association with CD. pyoderma gangrenosum occurs more often in patients with UC. Other dermatological entities in patients with CD are: aphthotic stomatitis, gingivitis, cheilitis, psoriasis.")
17
Extraintestinální manifestace
oči - záněty uvey, corney, retiny, optického nervu - u dětí velmi vzácné - katarakta, glaukom (nežádoucí účinky léčby steroidy) skeletální systém - osteoporóza cataract and glaucoma are more frequent side effects of steroid therapy. The most important extraintestinal manifestation affecting the skeletal system is osteoporosis. The osteoporosis may be due (particularly in CD) either to the disease itself or may be due to therapy. regular monitoring of bone density is essential. Lateral thoracic spine in a patient with severe osteoporosis. The spine appears diffusely osteopenic, and an insufficiency fracture of one of the thoracic vertebral bodies is noted.
 skeletální systém - osteoporóza. cataract and glaucoma are more frequent side effects of steroid therapy. The most important extraintestinal manifestation affecting the skeletal system is osteoporosis. The osteoporosis may be due (particularly in CD) either to the disease itself or may be due to therapy. regular monitoring of bone density is essential. Lateral thoracic spine in a patient with severe osteoporosis. The spine appears diffusely osteopenic, and an insufficiency fracture of one of the thoracic vertebral bodies is noted.")
18
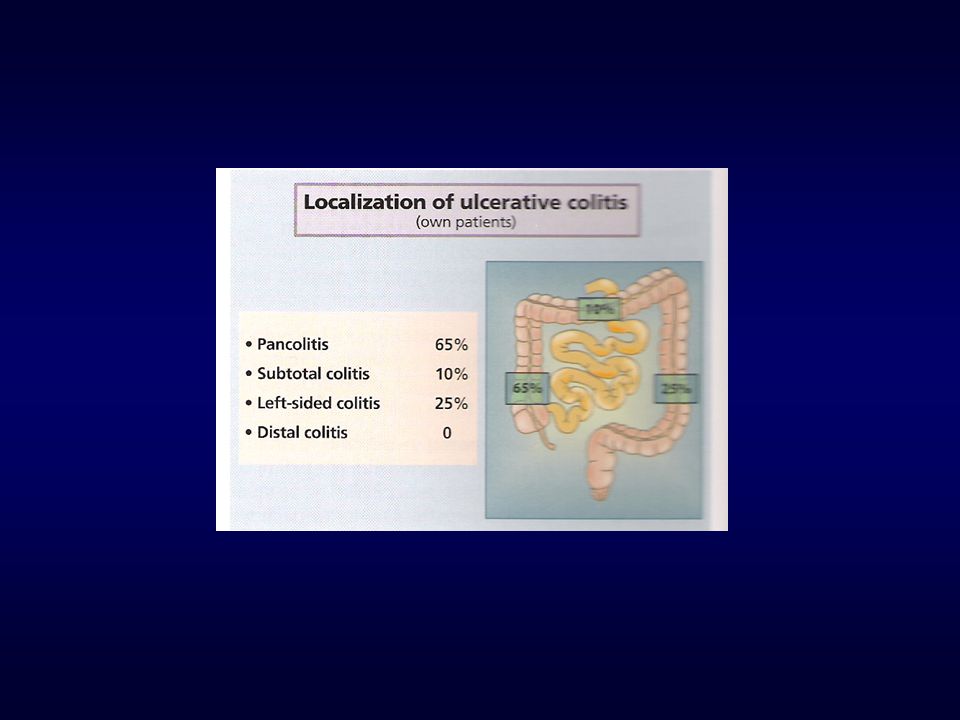
Ulcerózní kolitida vždy postihuje rektum a šíří se proximálně do ostatních částí tlustého střeva ulcerózní proktitida - postiženo rektum pankolitida - postiženo celé tlusté střevo zánět postihuje sliznici postižení je difůzní Disease virtually always begins in the rectum and extends proximally for a variable distatnce. When it is lacalized to the rectum, the disease is ulcerative proctitis. Disease involving the entire colon in pancolitis. About 30% of children who present with ulcerative proctitis experience proximal spread of the disease. UC is rarely been noted to present in infancy.Dietary protein intolerance (cows milk protein) may be easily misdiagnosed as UC.
 may be easily misdiagnosed as UC.")
20
Crohnova nemoc postihuje kteroukoliv část zažívacího traktu od dutiny ústní až po anus segmentální postižení skip oblasti (úseky nepostižené ostře ohraničené od postižených) postižení transmurální (celá stěna) forma - zánětlivá, infiltrující stenozující fistulující
 postižení transmurální (celá stěna) forma - zánětlivá, infiltrující - stenozující - fistulující.")
21
Among children with CD, the initial presentations most commonly involve ileum and colon (ileocolitis). But may involve the small bowel alone of colon alone (granulomatous colitis)
")
22
NSZ - odlišnosti CD postihuje:
kteroukoliv část trávicí trubice od úst až po anus, nejčastěji TI celou stěnu segmentálně UC postihuje: rektum a může postupovat aborálním směrem až do céka sliznici difůzně

23
Diagnóza NSZ anamnéza fyzikální vyšetření laboratorní vyšetření
diagnostický ultrazvuk břicha (stěna střevní) endoskopie + biopsie (flexibilní rektosigmoideoskopie, ezofagogastroduodenoskopie, koloskopie) histologické vyšetření bioptických vzorků radiologie The methods for establishing the diagnosis of IBD in children are identical to those used in adults patients. they are sumarized in table. It is usually possible to distinquish between UC and CD by the history, clinical presentation and endoscopic, histopathologic and radiologic findigs
 endoskopie + biopsie (flexibilní rektosigmoideoskopie, ezofagogastroduodenoskopie, koloskopie) histologické vyšetření bioptických vzorků. radiologie. The methods for establishing the diagnosis of IBD in children are identical to those used in adults patients. they are sumarized in table. It is usually possible to distinquish between UC and CD by the history, clinical presentation and endoscopic, histopathologic and radiologic findigs.")
24
Anamnestické údaje suspektní z diagnózy NSZ
příznaky jsou vleklé (chronické) bolest břicha průjem, někdy s krví hmotnostní úbytek, neprospívání opoždění růstu, puberty, amenorhea únava, omezení aktivit
 bolest břicha. průjem, někdy s krví. hmotnostní úbytek, neprospívání. opoždění růstu, puberty, amenorhea. únava, omezení aktivit.")
25
Anamnestické údaje suspektní z diagnózy NSZ
Pacienti s triádou bolesti břicha průjem neprospívání (hmotnostní úbytek, retardace růstu) vždy podezřelí z NSZ
 vždy podezřelí z NSZ.")
26
Fyzikální vyšetření antropometrické parametry (výška, hmotnost/věk, úplná výšková křivka k dokumentaci růstové rychlosti, hodnocení puberty dle Tannera) - pokles v percentilových pásmech nebo umístění pod 3.percentilem spolu se zpomalením (zástavou) růstové rychlosti – rozpoznání nemoci v časném stadiu ústní dutina (afty, gingivitida,…) kůže, klouby palpace břicha (rezistence) per rektum (fistule, perianální dermatitida,…)
 - pokles v percentilových pásmech nebo umístění pod 3.percentilem spolu se zpomalením (zástavou) růstové rychlosti – rozpoznání nemoci v časném stadiu. ústní dutina (afty, gingivitida,…) kůže, klouby. palpace břicha (rezistence) per rektum (fistule, perianální dermatitida,…)")
27
Perianální oblast u pacienta s CD
Chronic anal fissure at 5 o clock position with associated marisca in a patient with CD. Well developed marisca in the perianal region.

28
Fyzikální vyšetření suspektní z diagnózy NSZ
Pacienti s píštělemi a fisurami mimo č. 6 a 12 a enterorhagií podezřelí z NSZ a mají být endoskopováni

29
Laboratorní vyšetření
FW, CRP Hb, leukocyty, trombocyty, MCV sérové železo, ferritin, sTR CB, albumin, prealbumin ALT, AST, GMT, ALP, urea, kreatinin, S-amylasa, S-lipasa sérové elektrolyty, osmolalita m+s, kultivace moči stolice kultivace, paraziti, OK, Clostridium toxin Widal, yerzinie, chlamydie ANCA, ASCA, IgGAME Differentiation of CD and UC on the basis of the laboratory testing alone is difficult, antibody such as pANCA - increased in UC and ASCA (increased in CD) can help in individual cases In patients with CD - usually erythrocyte sedimentation rate (ESR), C- reactive protein and platelet level are icreased, we usually seen dicrese in TP (total protein level), albumin and prealbumin (nutritional parameters), sideropenic anemia in laboratory examination. In patients with UC with mild stage the laboratory testing usually could be normal.
 can help in individual cases. In patients with CD - usually erythrocyte sedimentation rate (ESR), C- reactive protein and platelet level are icreased, we usually seen dicrese in TP (total protein level), albumin and prealbumin (nutritional parameters), sideropenic anemia in laboratory examination. In patients with UC with mild stage the laboratory testing usually could be normal.")
30
Diagnostický ultrazvuk stěny střevní - ztluštění střevní stěny
In patients in whom the history and the result of the physical examinations suggest IBD, the ultrasound finding of thickening of the intestinal wall will furter support the diagnosis. But the main use of ultrasound is more in therapeutic monitoring and less in initial diagnosis of IBD.

31
Endoskopie s histologií u CD
EGD, koloskopie s terminální ileoskopií (v analgosedaci nebo CA) biopsie histologie - epiteloidní granulomy (50% pacientů) The next step in conferm diagnosis is endoscopy and histologic examination. EGD should be performed at the time of colonoscopy under brief or general anesthesia. The most important are stepped biopsies, because diagnosis of CD is confirmed when epitheloid cell or microgranulomas are found. They are found in over 50% of cases.
 biopsie. histologie - epiteloidní granulomy (50% pacientů) The next step in conferm diagnosis is endoscopy and histologic examination. EGD should be performed at the time of colonoscopy under brief or general anesthesia. The most important are stepped biopsies, because diagnosis of CD is confirmed when epitheloid cell or microgranulomas are found. They are found in over 50% of cases.")
32
normální ileocekální oblast
terminální ileitida

33
normální tračník Crohnovská kolitida

34
Endoskopie a histologie u UC
rektoskopie kompletní koloskopie (určení extenze nemoci a odebrání bioptických vzorků pro histologické vyšetření) histologie - akutní nebo chronický zánět Endoscopic work up can commence with a brief proctoscopy, because UC spreds continuously form distal to proximal within the colon If proctoscopy findings are pathologic, a complete colonoscopy is indicated in order to determine the extent of the disease and to obtain tissue samples for histologic study. If proctoscopy findings are normal there is a very high probability that UC is not present
 histologie - akutní nebo chronický zánět. Endoscopic work up can commence with a brief proctoscopy, because UC spreds continuously form distal to proximal within the colon. If proctoscopy findings are pathologic, a complete colonoscopy is indicated in order to determine the extent of the disease and to obtain tissue samples for histologic study. If proctoscopy findings are normal there is a very high probability that UC is not present.")
35
ulcerózní kolitida

36
Radiologické vyšetření
CD tenké střevo - enteroklýza - pasáž tlusté střevo - irrigografie UC - irrigografie

37
Radiologické vyšetření
CD UC Small bowel double contrast examination in patients with late stage of CD - ileocecal area, severe stenose of ileum with prestenotic dilatation. Colon - irrigation examination - early stage of UC Large ulcers in UC in colon Pseudopolyp in lienal flexure in UC

38
Diferenciální diagnóza NSZ
infekční enteropatie - virové, bakteriální, parazitární potravinová alergie hemolyticko - uremický syndrom Hennoch Schonlein purpura radiační proktitida The major conditions to exclude are infectious diseases. A history of contact with others with gastroenteritis is important. every child with suspicion for IBD should have stool cultured for enteric pathogens, stool evaluation for parasites, and serologis studies. One but better 3 stool samples are noted. In the setting of antibiotic use, pseudomembranous colitis to Clostridium difficile should be considered yerzinia may couse many of the radiologic and endoscopic findings in the distal small bowel that are seen in Crohn disease. In some cases infectious gastroenteritis may precede the development of IBD gastrointestinal tuberculosis is rare but can mimic CD. small bowell lymphoma may mimic CD growth failure may be the only manifestation of Crohn disease, other disorders such as growth hormone deficiency or gluten sensitive enteropathy must be considered

39
Diferenciální diagnóza NSZ
poruchy příjmu potravy (mentální anorexie, bulimie) lymfom tenkého střeva deficit STH gluten sensitivní enteropatie (celiakie) juvenilní revmatoidní artritida hematologická onemocnění (leukemie) chronické granulomatózní onemocnění
 lymfom tenkého střeva. deficit STH. gluten sensitivní enteropatie (celiakie) juvenilní revmatoidní artritida. hematologická onemocnění (leukemie) chronické granulomatózní onemocnění.")
40
Léčba NSZ Konzervativní nebo chirurgická Cíl léčby dosáhnout remise
zajistit věkově odpovídající somatický a psychosociální vývoj zabránit komplikacím

41
Léčba NSZ Léčba závisí na typu nemoci (CD, UC)
aktivitě nemoci (indexy aktivity, PCDAI, UCAI) mírná, střědní, vysoká aktivita lokalizaci nemoci
 mírná, střědní, vysoká aktivita. lokalizaci nemoci.")
42
Aktivita u UC

43
Konzervativní léčba vychází ze zkušeností a studií provedených u dospělých pacientů s NSZ malý počet kontrolovaných studií u dětí monoterapie nebo rozmanité kombinace léků The drugd listed in the previous table can be used as monotherapy or in various combinations according to the individual patients needs. The therapy of IBD in each patient must be individually adapted to the patient.

44
Medikamentózní léčba NSZ
In patients with involvement of distal bowel segments, local therapy is preferable to systemic therapy because of less severe side effects.

45
Glukokortikosteroidy
indikace 5-ASA nebo SASP neefektivní (CD, UC) postižení horní části GI traktu u CD (jícen až jejunum) extraintestinální manifestace u CD nejzávažnější vedlejší účinek léčby – růstová retardace, osteoporóza budesonid - topicky účinný steroid, počet vedlejších účinků podstatně nižší GCS are indicated in patients in whom 5-ASA or SASP are inadequate, and in those with involvement of the upper GI tract (esophagus to jejunem) and/or extraintestinal manifestation The most important side effect od GCS is growth retardation Budesonid is a topically active steroid This drug is metabolised on the first passage through the liver The rate of side effects is much lower than with the classical glucocorticoids. The goal is to taper the alternate day dose within 1-3months.
 postižení horní části GI traktu u CD (jícen až jejunum) extraintestinální manifestace u CD. nejzávažnější vedlejší účinek léčby – růstová retardace, osteoporóza. budesonid - topicky účinný steroid, počet vedlejších účinků podstatně nižší. GCS are indicated in patients in whom 5-ASA or SASP are inadequate, and in those with involvement of the upper GI tract (esophagus to jejunem) and/or extraintestinal manifestation. The most important side effect od GCS is growth retardation. Budesonid is a topically active steroid. This drug is metabolised on the first passage through the liver. The rate of side effects is much lower than with the classical glucocorticoids. The goal is to taper the alternate day dose within 1-3months.")
46
Azathioprine, 6-MP indikace vedlejší účinky
chronické aktivní onemocnění (CD, UC) fistulující forma CD vedlejší účinky horečka, pankreatitida, GI intolerance, častější infekce pankreatitida – celoživotní kontraindikace pravidelný laboratorní monitoring (leukocyty, amyláza v séru) nástup účinku s latencí 2-9 měsíců Azathioprine or 6-MP we can used in patients with chronic active disease to keep remission. Further indication is the presens of fistulae. Side effects are: fever, pancreatitis, GI intolerance, increased infections duo to decrease WBC (white blood count) Pancreatitis represents a life long contraindication for azathioprine. Regular laboratory monitoring during therapy is useful (WBC, serum amylasa) Disadvantage - drug effects usually appear within 2-6 months.
 fistulující forma CD. vedlejší účinky. horečka, pankreatitida, GI intolerance, častější infekce. pankreatitida – celoživotní kontraindikace. pravidelný laboratorní monitoring (leukocyty, amyláza v séru) nástup účinku s latencí 2-9 měsíců. Azathioprine or 6-MP we can used in patients with chronic active disease to keep remission. Further indication is the presens of fistulae. Side effects are: fever, pancreatitis, GI intolerance, increased infections duo to decrease WBC (white blood count) Pancreatitis represents a life long contraindication for azathioprine. Regular laboratory monitoring during therapy is useful (WBC, serum amylasa) Disadvantage - drug effects usually appear within 2-6 months.")
47
Antibiotika - metronidazol
hypotéza některé bakteriální antigeny jsou schopné spustit patologickou imunitní odpověď ve střevní sliznici indikace postižení tračníku perianální fistule léčba je dlouhodobá The use of antibiotics in the treatment of IBD is based on the hypothesis, that some bacterial antigen has triggered pathologic immune response in the intestinal mucosa Disease lokalized to the colon and in the treatment of fistulae Long term therapy.

48
Cyclosporin A, antiTNF (infliximab)
léčba akutní ataky UC vedlejší účinky - hypertrichóza, gingivální hyperplázie antiTNF indikace u CD pacient refrakterní na léčbu GCS a IS fistulující forma CD chimerická monoklonální protilátka proti TNF, nejdůležitější prozánětlivý cytokin The use of antibiotics in the treatment of IBD is based on the hypothesis, that some bacterial antigen has triggered pathologic immune response in the intestinal mucosa Disease lokalized to the colon and in the treatment of fistulae Long term therapy.

49
Vedlejší účinky léků užívaných v léčbě NSZ

50
Léčba CD a UC s vysokou aktivitou (fulminantní průběh)
parenterální tekutiny a elektrolyty parenterální a enterální výživa GCS (solumedrol) 1-1,5mg/kg/d IV metronidazol 10-20mg/kg/d IV bez efektu 5-7 dní cyclosporin A PPI, KCl, racionální hemoterapie
 1-1,5mg/kg/d IV. metronidazol 10-20mg/kg/d IV. bez efektu 5-7 dní cyclosporin A. PPI, KCl, racionální hemoterapie.")
51
Nutriční enterální léčba (NEL) u CD
NEL je srovnatelná s GCS ve svém protizánětlivém účinku nemá žádné nepříznivé vedlejší účinky! mechanismus působení? redukce prozánětlivých slizničních cytokinů (IL-1, IL-10, INF) NET (elemental, semielemental, polymeric diets) in patients with CD. Most often Fresubin or Nutridrink NET is comparable to GCS in terms of anti-inflammatory action, but have no side effects!!! A result of this therapy is a reduction in the pro-inflammatory mucosal cytokines (IL-1, IL-10, INF gama. Enteral therapy is continued for 4-8weeks. During this time nothing is allowed by mouth with the exception of water The amount of the NET corresponds to patients caloric requirements plus any existing deficits Formula can be applied through a gastric tube The efficacy the NET in patients with disease involving the distal colon remains controversial No study has shown a beneficila effect for NET in patients with UC.
 NET (elemental, semielemental, polymeric diets) in patients with CD. Most often Fresubin or Nutridrink. NET is comparable to GCS in terms of anti-inflammatory action, but have no side effects!!! A result of this therapy is a reduction in the pro-inflammatory mucosal cytokines (IL-1, IL-10, INF gama. Enteral therapy is continued for 4-8weeks. During this time nothing is allowed by mouth with the exception of water. The amount of the NET corresponds to patients caloric requirements plus any existing deficits. Formula can be applied through a gastric tube. The efficacy the NET in patients with disease involving the distal colon remains controversial. No study has shown a beneficila effect for NET in patients with UC.")
52
Nutriční enterální léčba (NEL) u CD
NEL podávána 4-8 týdnů pacienti mohou pouze vodu nebo čaj množství NEL odpovídá kalorické potřebě pacienta + doplnění existujícího deficitu perorálně (sipping), PEG, PEG/J, PEJ účinnost u Crohnovské kolitidy je kontroversní NEL není účinná u pacientů s UC
, PEG, PEG/J, PEJ. účinnost u Crohnovské kolitidy je kontroversní. NEL není účinná u pacientů s UC.")
53
Probiotika žijící mikroorganismy pozitivní účinek u pacientů s NSZ
Lactobacillus GG, E. Coli Nissle, Saccharomyces Baulardii

54
Vitamíny, stopové prvky
Substituce vitamínu B12 (ileocekální resekce, vysoká aktivita zánětu v ileocekální oblasti) vitamínů B6, A, E, D, kyseliny listové železa, kalcia, magnesia zinku, selenu modulární dietetika (Fantomalt, Protifar) enterální výživa (Fresubin, Nutridrink)
 vitamínů B6, A, E, D, kyseliny listové. železa, kalcia, magnesia. zinku, selenu. modulární dietetika (Fantomalt, Protifar) enterální výživa (Fresubin, Nutridrink)")
55
psychoterapie je jednou z důležitých částí léčby NSZ
NSZ jsou chronická celoživotní onemocnění s obdobím remisí a nepředvídatelných exacerbací velmi stresující pro postižené dítě a jeho rodinu (rodiče, sourozence) psychoterapie je jednou z důležitých částí léčby NSZ
 psychoterapie je jednou z důležitých částí léčby NSZ.")
56
Chirurgická léčba u CD riziko relapů syndrom krátkého střeva
% pacientů indikace rezistence k medikamentózní léčbě chronický subileus (striktury) zpomalení/zástava růstu, puberty fistule, abscesy, perforace nekontrolovatelné krvácení In pediatric patients with UC surgery is rarely performed. But is much more frequently required in children with CD. Surgery in CD is always associated with the risk of relaps, leading finally to the short bowel syndrom because of the danger of reccurence the determination of indication for surgery is very strict and includes following considerations: Chronic disease activity remains the most common indication for surgery therapy. In patients also suffering from growth disturbances, the decision to recommend surgical treatment should not be delayd. Beneficial efects of surgery on growth in prepubertal patients with IBDare clearly established
 zpomalení/zástava růstu, puberty. fistule, abscesy, perforace. nekontrolovatelné krvácení. In pediatric patients with UC surgery is rarely performed. But is much more frequently required in children with CD. Surgery in CD is always associated with the risk of relaps, leading finally to the short bowel syndrom. because of the danger of reccurence the determination of indication for surgery is very strict and includes following considerations: Chronic disease activity remains the most common indication for surgery therapy. In patients also suffering from growth disturbances, the decision to recommend surgical treatment should not be delayd. Beneficial efects of surgery on growth in prepubertal patients with IBDare clearly established.")
57
Chirurgická léčba u CD postoperační komplikace 17% pacientů
stenóza v anastomóze vznik fistulí absces

58
Chirurgická léčba u UC vzácně nutná indikace nekontrolované krvácení
toxické megakolon 3 základní chirurgické přístupy totální kolektomie s ileostomií kolektomie s ileoanální anastomózou kolektomie s proktomukosektomií a vytvořením ileoanálního pauche The indication for surgery is almost always uncotrolable bleedings

59
Ambulantní péče o pacienty s NSZ
při každé ambulantní kontrole stanovení nutričního stav pacienta antropometrické parametry tělesná hmotnost, výška (percentilové grafy) růstová rychlost body mass index BMI = tělesná hmotnost (kg)/výška (m2) puberta (Tanner skore)
 růstová rychlost. body mass index BMI = tělesná hmotnost (kg)/výška (m2) puberta (Tanner skore)")
60
Ambulantní péče o pacienty s NSZ
určení klinické a laboratorní aktivity, stavu nutrice, NÚ užívaných léků FW, KO+dif., CRP sérové železo, ferritin, sTR CB, albumin, prealbumin ALT, AST, GMT, ALP, amyláza v séru kalcium, fosfor, PTH magnesium, Quick, vitamin A, E, B12, kyselina listová

61
Ambulantní péče o pacienty s NSZ
jednou za rok jídelníček za 3 dny RTG levého zápěstí – kostní věk DEXA (dual energy X-ray absorbimetry) k urční BMD ultrazvuk břicha – stěna střevní endoskopie, RTG dle průběhu onemocnění
 k urční BMD. ultrazvuk břicha – stěna střevní. endoskopie, RTG dle průběhu onemocnění.")
62
Antropometrické parametry – výška/věk
Dg CF Dg. Crohnovy nemoci Somatogram of the patients with CD showing an abnormal pattern of growth. 6300g

63
Antropometrické parametry – hmotnost/věk
Dg CF 6300g Dg Crohnovy nemoci

64
UC - riziko karcinomu tlustého střeva
pankolitida – riziko ca. se po 8-10 letech trvání UC o 0,5-1%/rok levostranný typ - riziko ca. se zvyšuje po 20 letech trvání UC proktokolitida – riziko ca. jako v běžné populaci vzniku karcinomu předchází dysplastické změny sliznice prevence karcinomu tlustého střeva - kontrolní koloskopie v intervalu 1 rok s etážovitým odběrem biopsií tračníku a 10cm

65
Děkuji za pozornost

Podobné prezentace










 MYELOM.>")





 Spinoceluární karcinom (oblast horních 2/3 jícnu) Pohlaví: výskyt 7x více.>")



