Stáhnout prezentaci
Prezentace se nahrává, počkejte prosím

1
Zdravotní politika (JSM601) UK, Fakulta sociálních věd Katedra veřejné a sociální politiky Petr Háva Téma ZP2: Zdraví a nemoc ve společnosti Determinanty zdraví a nemoci, měření zdraví a nemoci, strategie a cíle zdravotní politiky

2
ZP2: Zdraví a nemoc ve společnosti
Úvodní informace: Nemoc jako sociální problém, sociologie medicíny Prezentace: Teoretická východiska Zdraví, nemoc, determinanty zdraví a nemoci, klasifikace nemocí Měření zdraví a jeho determinant Výzkum zdraví u populačních skupin Výzkum determinant zdraví Měření nemoci (individuální a populační přístupy) Klasifikace nemocí (Mezinárodní klasifikace nemocí) Diagnostika jednotlivých pacientů Epidemiologie (populační přístupy) Populační genetika Případová studie: Analýza vývoje zdravotního stavu v Jihočeském kraji Program: Zdraví 2020
 Klasifikace nemocí (Mezinárodní klasifikace nemocí) Diagnostika jednotlivých pacientů. Epidemiologie (populační přístupy) Populační genetika. Případová studie: Analýza vývoje zdravotního stavu v Jihočeském kraji. Program: Zdraví")
3
Vstupní informace: Nemoc jako sociální problém
Proč je nemoc sociálním problémem? Z hlediska důsledků nemocnosti pro společnost Chronická onemocnění se sníženou soběstačností, vyžadující sociální služby/péči, omezená participace na společenském dění (duševní nemoci, srdeční a cévní, pohybová, invalidita) Vazby na délku působení na trhu práce Z hlediska důsledků fungování společnosti pro jedince Kontrola determinant zdraví a nemoci Vliv na životní styl, životní prostředí Vývoj nemocnosti, celkové zátěže nemocemi, úmrtnost
 Vazby na délku působení na trhu práce. Z hlediska důsledků fungování společnosti pro jedince. Kontrola determinant zdraví a nemoci. Vliv na životní styl, životní prostředí. Vývoj nemocnosti, celkové zátěže nemocemi, úmrtnost.")
4
Zdraví a nemoc ve společnosti
Sociální důsledky nemocnosti, hodnocení výsledků Společenské problémy, agendy a cíle politiky, Veřejná politika Veřejná správa Právní normy Financování a úhrady Nákup služeb (zdraví) Smluvní vztahy NABÍDKA Zdravotnické služby AMBULANTNÍ LŮŽKOVÉ LÉKÁRNY OSTATNÍ Medicínské technologie zdravotnické prostředky Veřejné zdraví Podpora zdraví POTŘEBY POPTÁVKA VÝSLEDKY Kvalita života Zdravotní stav (zátěž nemocemi) Společnost Výzkum Vzdělávání SPOTŘEBA
 Smluvní vztahy. NABÍDKA. Zdravotnické služby. AMBULANTNÍ. LŮŽKOVÉ. LÉKÁRNY. OSTATNÍ. Medicínské technologie zdravotnické prostředky. Veřejné zdraví. Podpora zdraví. POTŘEBY. POPTÁVKA. VÝSLEDKY. Kvalita života. Zdravotní stav (zátěž nemocemi) Společnost. Výzkum. Vzdělávání. SPOTŘEBA.")
5
Myšlenková mapa 3.Nové teoretické koncepty, paradigmatický posun
Od biologicko-medicínského k sociálně-psychologickému 5.Změna přístupu zdravotní politiky pro 21. století 4.Praktické využití cestou programů podpory zdraví 1.Zdraví a nemoc ve společnosti 2.Determinanty zdraví a nemoci, základní teorie 9.Veřejné zdraví 6.medicína 7.Molekulární medicína 10.Analýzy a výzkum zdravotního stavu (epidemiologie, demografie, zátěž nemocemi, nerovnosti) 14.Výzkum determinant zdraví a nemoci Sociologické výzkumy Hodnocení společenských důsledků 8.Evaluační výzkumy, řízení kvality VÝSLEDKY 11.Celostní hodnotící přístup 12.Lidská práva, rovnost práv 13.Spravedlnost
 14.Výzkum determinant zdraví a nemoci. Sociologické výzkumy. Hodnocení společenských důsledků. 8.Evaluační výzkumy, řízení kvality. VÝSLEDKY. 11.Celostní hodnotící přístup. 12.Lidská práva, rovnost práv. 13.Spravedlnost.")
6
Nemoc jako sociální problém
Problémy v rodinách Potřeba neformální péče Zátěž pro rodiny V sousedním Německu a Rakousku postupně tyto problémy vedly ke vzniku samostatného pojištění na poskytování sociální péče Čeká nás v ČR takové rozhodnutí?? Sociální izolace, vyloučení, marginalizace rizikových skupin, skupin s vyšší zátěží nemocemi Mezera ve zdraví. Ve státech střední a východní Evropy můžeme sledovat dosti odchylný vývoj úmrtnosti ve starších věkových skupinách Komplementární pohled: Investice do zdraví

7
Nemoc jako sociální problém
Konverguje vývoj zdravotního stavu ve státech střední a východní Evropy (v nových zemích) s vývojem ve starých zemích (EU15)? Jaké jsou příčiny existujících rozdílů a jaká data máme k dispozici?
 s vývojem ve starých zemích (EU15) Jaké jsou příčiny existujících rozdílů a jaká data máme k dispozici")
8
Výchozí otázky Je problém zátěže české populace nemocemi všemi tvůrci zdravotní politiky (a obecně politiky) dostatečně vnímán, nepřevažuje u nich orientace na problémy financování zdravotnictví? Existuje taková situace také na mezinárodní úrovni? (WHO, UN, EU, OECD) a existuje rozdíl v postojích politiků mezi ČR a jinými státy či nadnárodními organizacemi? Lze zdravotní stav zlepšit cestou lepšího fungování zdravotnictví na bázi trhu, samotných zdravotnických služeb a jejich financování nebo jde o složitější procesy? Je dostačující individuální přístup k pacientům nebo hraje roli také populační přístup. Jaké jsou naše možnosti kontroly vývoje zdraví populací a jedinců?
 dostatečně vnímán, nepřevažuje u nich orientace na problémy financování zdravotnictví Existuje taková situace také na mezinárodní úrovni (WHO, UN, EU, OECD) a existuje rozdíl v postojích politiků mezi ČR a jinými státy či nadnárodními organizacemi Lze zdravotní stav zlepšit cestou lepšího fungování zdravotnictví na bázi trhu, samotných zdravotnických služeb a jejich financování nebo jde o složitější procesy Je dostačující individuální přístup k pacientům nebo hraje roli také populační přístup. Jaké jsou naše možnosti kontroly vývoje zdraví populací a jedinců")
9
Cíl přednášky Vývoj zdraví a zdravotního stavu jako zásadního východiska (a současně i hodnotícího kritéria úspěšnosti) tvorby a realizace zdravotní politiky Problém: ČR – rozdíl v ukazatelích zdravotního stavu a determinant zdraví (úmrtnost, nemocnost, rizikové faktory jako např. spotřeba tabáku) oproti EU15 - „HEALTH GAP“ Cílem této přednášky nejsou detaily jednotlivých vědních disciplín, ale chápání souvisejících společenských procesů: zdraví a jeho determinanty, možnosti měření a hodnocení těchto procesů), přehled zdrojů dat
 tvorby a realizace zdravotní politiky. Problém: ČR – rozdíl v ukazatelích zdravotního stavu a determinant zdraví (úmrtnost, nemocnost, rizikové faktory jako např. spotřeba tabáku) oproti EU15 - „HEALTH GAP Cílem této přednášky nejsou detaily jednotlivých vědních disciplín, ale chápání souvisejících společenských procesů: zdraví a jeho determinanty, možnosti měření a hodnocení těchto procesů), přehled zdrojů dat.")
10
1. Teoretická východiska
Vědní disciplíny Koncepty Zdraví a nemoc Determinanty zdraví Burden of disease Healthy life years Komprese nemocnosti Kvalita života Veřejné zdraví (public health) Podpora zdraví Epidemiologie Medicína Demografie Sociologie Antropologie Psychologie
 Podpora zdraví. Epidemiologie. Medicína. Demografie. Sociologie. Antropologie. Psychologie.")
11
Teorie – realita - politika
Jaké si klademe otázky? Stačí nám popisnost? Pozitivismus, rozšíření o normativní přístupy Snažíme se lépe porozumět realitě? Fenomenologie, veřejné zdraví, podpora zdraví Jak aplikujeme poznatky v politice Kontext globalizace: Různé zájmy sociálních aktérů znamenají odlišné interpretace vlastních cílů a situací v globálních vztazích i v různých typech sociálních prostorů (Suša 2010)
")
12
Vědecká „produkce“ teoretických poznatků
Teorie Vysvětlení vztahů příčina účinek účinky příčiny METODOLOGIE Pozitivismus postpozitivismus Metody pro zpracování dat Metody, výběr metod, Metody, výběr metod Reálné vztahy příčina-účinek (události, procesy) Existující příčiny Reálné výsledky, problémy REALITA Výzkumný problém, jeho vstupní analýza
 Existující. příčiny. Reálné výsledky, problémy. REALITA. Výzkumný problém, jeho vstupní analýza.")
13
1.1 Teoretická východiska (zdraví*, nemoc)
ZDRAVÍ je stav úplné tělesné, duševní a sociální pohody a ne pouze nepřítomnost nemoci (definice SZO, 1948) ZDRAVÍ je relativně optimální stav tělesné, duševní a sociální pohody při zachování všech životních funkcí, společenských rolí a schopnosti organismu přizpůsobit se měnícím podmínkám prostředí Health This article is about the human condition. For other uses, see Health (disambiguation). Jump to: navigation, search From Wikipedia, the free encyclopedia Health is the level of functional and (or) metabolic efficiency of a living being. In humans, it is the general condition of a person in mind, body and spirit, usually meaning to be free from illness, injury or pain (as in “good health” or “healthy”).[1] The World Health Organization (WHO) defined health in its broader sense in 1946 as "a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity."[2][3] Although this definition has been subject to controversy, in particular as having a lack of operational value and the problem created by use of the word "complete", it remains the most enduring.[4][5] Classification systems such as the WHO Family of International Classifications, including the International Classification of Functioning, Disability and Health (ICF) and the International Classification of Diseases (ICD), are commonly used to define and measure the components of health. The Star of Life. The maintenance and promotion of health is achieved through different combination of physical, mental, and social well-being, together sometimes referred to as the “health triangle”.[6][7] The WHO's 1986 Ottawa Charter for Health Promotion furthered that health is not just a state, but also "a resource for everyday life, not the objective of living. Health is a positive concept emphasizing social and personal resources, as well as physical capacities."[8] Systematic activities to prevent or cure health problems and promote good health in humans are delivered by health care providers. Applications with regard to animal health are covered by the veterinary sciences. The term "healthy" is also widely used in the context of many types of non-living organizations and their impacts for the benefit of humans, such as in the sense of healthy communities, healthy cities or healthy environments. In addition to health care interventions and a person's surroundings, a number of other factors are known to influence the health status of individuals, including their background, lifestyle, and economic and social conditions; these are referred to as "determinants of health". 1 Determinants of health [hide] Contents 2 Maintaining health 2.2 Role of public health 2.1 Role of science in health 2.3 Self care strategies 5 External links 4 References 3 See also Generally, the context in which an individual lives is of great importance on health status and quality of life. It is increasingly recognized that health is maintained and improved not only through the advancement and application of health science, but also through the efforts and intelligent lifestyle choices of the individual and society. According to the World Health Organization, the main determinants of health include the social and economic environment, the physical environment, and the person's individual characteristics and behaviors.[9] See also: Social determinants of health and Risk factor [edit] Determinants of health Social support networks Income and social status More specifically, key factors that have been found to influence whether people are healthy or unhealthy include:[9][10][11] Education and literacy Physical environments Social environments Employment/working conditions Biology and genetics Healthy child development Personal health practices and coping skills Health care services An increasing number of studies and reports from different organizations and contexts examine the linkages between health and different factors, including lifestyles, environments, health care organization, and health policy - such as the 1974 Lalonde report from Canada[11]; the Alameda County Study in California[12]; and the series of World Health Reports of the World Health Organization, which focuses on global health issues including access to health care and improving public health outcomes, especially in developing countries.[13] Culture Gender Environmental: all matters related to health external to the human body, and over which the individual has little or no control; Lifestyle: the aggregation of personal decisions (i.e. over which the individual has control) that can be said to contribute to, or cause, illness or death; The concept of the "health field", as distinct from medical care, emerged from the Lalonde report from Canada. The report identified three interdependent fields as key determinants of an individual's health. These are:[11] Focusing more on lifestyle issues and their relationships with functional health, data from the Alameda County Study suggested that people can improve their health via exercise, enough sleep, maintaining a healthy body weight, limiting alcohol use, and avoiding smoking.[12] The ability to adapt and to self manage have been suggested as core components of human health.[14] Biomedical: all aspects of health, physical and mental, developed within the human body as influenced by genetic make-up. The environment is often cited as an important factor influencing the health status of individuals. This includes characteristics of the natural environment, the built environment, and the social environment. Factors such as clean water and air, adequate housing, and safe communities and roads all have been found to contribute to good health, especially the health of infants and children.[9][15] Some studies have shown that a lack of neighborhood recreational spaces including natural environment leads to lower levels of personal satisfaction and higher levels of obesity, linked to lower overall health and well being.[16] This suggests the positive health benefits of natural space in urban neighborhoods should be taken into account in public policy and land use. Genetics, or inherited traits from parents, also play a role in determining the health status of individuals and populations. This can encompass both the predisposition to certain diseases and health conditions, as well as the habits and behaviors individuals develop through the lifestyle of their families - also referred to as the "nature versus nurture" debate, in other words the role of factors which can or cannot be controlled. For example, genetics may play a role in the manner in which people cope with stress, either mental, emotional or physical. [edit] Role of science in health Achieving and maintaining health is an ongoing process, shaped by both the evolution of health care knowledge and practices, as well as personal strategies and organized interventions for staying healthy. [edit] Maintaining health Health science is the branch of science focused on health. There are two main approaches to health science: the study and research of the body and health-related issues to understand how humans (and animals) function; and the application of that knowledge to improve health and to prevent and cure diseases and other physical and mental impairments. The science builds on many sub fields, including biology, biochemistry, physics, epidemiology, pharmacology, medical sociology, and others. Applied health sciences endeavor to better understand and improve human health through applications in areas such as health education, biomedical engineering, biotechnology and public health. Main articles: Health science and Health care Organized interventions to improve health based on the principles and procedures developed through the health sciences are delivered among practitioners trained in medicine, nursing, nutrition, pharmacy, social work, psychology, physical therapy and other health care professions. Clinical practitioners focus mainly on the health of individuals, while public health practitioners consider the overall health of communities and populations. Workplace wellness programs are increasingly adopted by companies for their value in improving the health and well-being of their employees, as are school health services to improve the health and well-being of children. [edit] Role of public health Postage stamp, New Zealand, Public health has been promoted - and depicted - in a wide variety of ways. See also: Global health Main article: Public health Public health has been described as "the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and private, communities and individuals."[17] It is concerned with threats to the overall health of a community based on population health analysis. The population in question can be as small as a handful of people or as large as all the inhabitants of several continents (for instance, in the case of a pandemic). Public health has many sub-fields, but typically includes the interdisciplinary categories of epidemiology, biostatistics and health services. Environmental health, community health, behavioral health, and occupational health, are also important areas of public health. The focus of public health interventions is to prevent and manage diseases, injuries and other health conditions through surveillance of cases and the promotion of healthy behaviors, communities and environments. Its aim is preventing from happening or re-occurring health problems by implementing educational programs, developing policies, administering services, and conducting research.[18] In many cases, treating a disease or controlling a pathogen can be vital to preventing it in others, such as during an outbreak. Vaccination programs and distribution of condoms to prevent the spread of communicable diseases are examples of common preventive public health measures. Public health also takes several actions to limit the health disparities between different areas of the country, continent or world. The great issue is addressing access of individuals and communities to health care, in terms of financial, geographical or sociocultural constraints in access to and use of services. Applications of the public health system include areas of maternal and child health, health services administration, emergency response, and prevention and control of infectious and chronic diseases. The great positive impact of public health programs is widely acknowledged. Due in part to the policies and actions developed through public health, the 20th century registered a decrease of the mortality rates in infants and children and a continual increase in life expectancy in most parts of the world. For example, it is estimated that the life expectancy has increased for Americans by thirty years since 1900,[19] and worldwide by six years since 1990.[20] See also: Chronic care management, Social relation, and Stress management Main article: Self care [edit] Self care strategies Personal health depends partially on the active, passive, and assisted cues people observe and adopt about their own health. These include personal actions for preventing or minimizing the effects of a disease, usually a chronic condition, through integrative care. They also include personal hygiene practices to prevent infection and illness, such as bathing and washing hands with soap; brushing and flossing teeth; storing, preparing and handling food safely; and many others. The information gleaned from personal observations of daily living - such as about sleep patterns, exercise behavior, nutritional intake, and environmental features - may be used to inform personal decisions and actions (e.g., "I feel tired in the morning so I am going to try sleeping on a different pillow"), as well as clinical decisions and treatment plans (e.g., a patient who notices his or her shoes are tighter than usual may be having exacerbation of left-sided heart failure, and may require diuretic medication to reduce fluid overload).[21] Personal health also depends partially on the social structure of a person's life. The maintenance of strong social relationships, volunteering, and other social activities have been linked to positive mental health and even increased longevity. One American study among seniors over age 70 found that frequent volunteering was associated with reduced risk of dying compared with older persons who did not volunteer, regardless of physical health status.[22] Another study from Singapore reported that volunteering retirees had significantly better cognitive performance scores, fewer depressive symptoms, and better mental well-being and life satisfaction than non-volunteering retirees.[23] Prolonged psychological stress may negatively impact health, and has been cited as a factor in cognitive impairment with aging, depressive illness, and expression of disease.[24] Stress management is the application of methods to either reduce stress or increase tolerance to stress. Relaxation techniques are physical methods used to relieve stress. Psychological methods include cognitive therapy, meditation, and positive thinking which work by reducing response to stress. Improving relevant skills, such as problem solving and time management skills, reduces uncertainty and builds confidence, which also reduces the reaction to stress-causing situations where those skills are applicable. complete health information [edit] See also Global burden of disease Book: HealthWikipedia books are collections of articles that can be downloaded or ordered in print.Behavioral change theories Health and fitness portal Health care Health policy Health education Health care providers Primary health care Health workforce Health systems History of medicine Nutrition Leveraging Agriculture for Improving Nutrition and Health Healthy narcissism ^ Merriam-Webster. Dictionnary - "Health", accessed 21 April 2011. [edit] References One Health ^ World Health Organization [ WHO definition of Health], Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April 1948. ^ Jadad AR, O'Grady L. "How should health be defined?" BMJ 2008; 337:a ^ Callahan D. "The WHO definition of 'health'." The Hastings Center Studies, 1(3), ^ World Health Organization Constitution of the World Health Organization - Basic Documents, Forty-fifth edition, Supplement, October 2006. ^ World Health Organization Ottawa Charter for Health Promotion, adopted at the First International Conference on Health Promotion, Ottawa, 21 November WHO/HPR/HEP/95.1. ^ Nutter S The Health Triangle. Anchor Points, Inc. ^ Georgia State University Health Triangle Slides. ^ a b c World Health Organization. The determinants of health. Geneva. Accessed 12 May 2011. ^ a b Housman J, Dorman S "The Alameda County Study: A Systematic, Chronological Review" American Journal of Health Education; 36(5):302–308. ^ a b c Lalonde, Marc. "A New Perspective on the Health of Canadians." Ottawa: Minister of Supply and Services; 1974. ^ Public Health Agency of Canada. What Determines Health? Ottawa. Accessed 12 May 2011. ^ UNESCO. The UN World Water Development Report: Facts and Figures - Meeting basic needs. Accessed 12 May 2011. ^ Huber M et al. "How should we define health?" BMJ 2011;343 doi: /bmj.d4163 (Published 26 July 2011). Accessed 2 August 2011. ^ World Health Organization. The world health report. Geneva. ^ Bjork J et al. "Recreational Values of the Natural Environment in Relation to Neighborhood Satisfaction, Physical Activity, Obesity and Well being." J Epidemiol Community Health 2008;62:e2 ^ Association of Schools of Public Health. Impact of Public Health. Retrieved ^ Association of Schools of Public Health. What is Public Health? Retrieved ^ C.-E. A. Winslow “The Untilled Fields of Public Health,” Science, n.s. 51. ^ Harris AHS, Thoresen CE. "Volunteering is Associated with Delayed Mortality in Older People: Analysis of the Longitudinal Study of Aging." Journal of Health Psychology, 2005; 10(6): 739–752. ^ Robert Wood Johnson Foundation Health in Everyday Living. ^ World Health Organization. Life expectancy at birth, accessed 20 April 2011. ^ Schwingel A et al. "Continued work employment and volunteerism and mental well-being of older adults: Singapore longitudinal ageing studies." Age and Ageing, 2009; 38(5): Look up health in Wiktionary, the free dictionary.Wikiquote has a collection of quotations related to: HealthWorld Health and Organization [edit] External links ^ McEwen BS (2006). "Protective and damaging effects of stress mediators: central role of the brain". Dialogues Clin Neurosci 8 (4): 367–81. PMID OECD Health Statistics Health On the Net Foundation UK National Health Service Health-EU Portal, public health portal of the European Union Health and Medical Information from the University of Colorado
 ZDRAVÍ je relativně optimální stav tělesné, duševní a sociální pohody při zachování všech životních funkcí, společenských rolí a schopnosti organismu přizpůsobit se měnícím podmínkám prostředí. Health. This article is about the human condition. For other uses, see Health (disambiguation). Jump to: navigation, search. From Wikipedia, the free encyclopedia. Health is the level of functional and (or) metabolic efficiency of a living being. In humans, it is the general condition of a person in mind, body and spirit, usually meaning to be free from illness, injury or pain (as in good health or healthy ).[1] The World Health Organization (WHO) defined health in its broader sense in 1946 as a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity. [2][3] Although this definition has been subject to controversy, in particular as having a lack of operational value and the problem created by use of the word complete , it remains the most enduring.[4][5] Classification systems such as the WHO Family of International Classifications, including the International Classification of Functioning, Disability and Health (ICF) and the International Classification of Diseases (ICD), are commonly used to define and measure the components of health. The Star of Life. The maintenance and promotion of health is achieved through different combination of physical, mental, and social well-being, together sometimes referred to as the health triangle .[6][7] The WHO s 1986 Ottawa Charter for Health Promotion furthered that health is not just a state, but also a resource for everyday life, not the objective of living. Health is a positive concept emphasizing social and personal resources, as well as physical capacities. [8] Systematic activities to prevent or cure health problems and promote good health in humans are delivered by health care providers. Applications with regard to animal health are covered by the veterinary sciences. The term healthy is also widely used in the context of many types of non-living organizations and their impacts for the benefit of humans, such as in the sense of healthy communities, healthy cities or healthy environments. In addition to health care interventions and a person s surroundings, a number of other factors are known to influence the health status of individuals, including their background, lifestyle, and economic and social conditions; these are referred to as determinants of health . 1 Determinants of health. [hide] Contents. 2 Maintaining health. 2.2 Role of public health. 2.1 Role of science in health. 2.3 Self care strategies. 5 External links. 4 References. 3 See also. Generally, the context in which an individual lives is of great importance on health status and quality of life. It is increasingly recognized that health is maintained and improved not only through the advancement and application of health science, but also through the efforts and intelligent lifestyle choices of the individual and society. According to the World Health Organization, the main determinants of health include the social and economic environment, the physical environment, and the person s individual characteristics and behaviors.[9] See also: Social determinants of health and Risk factor. [edit] Determinants of health. Social support networks. Income and social status. More specifically, key factors that have been found to influence whether people are healthy or unhealthy include:[9][10][11] Education and literacy. Physical environments. Social environments. Employment/working conditions. Biology and genetics. Healthy child development. Personal health practices and coping skills. Health care services. An increasing number of studies and reports from different organizations and contexts examine the linkages between health and different factors, including lifestyles, environments, health care organization, and health policy - such as the 1974 Lalonde report from Canada[11]; the Alameda County Study in California[12]; and the series of World Health Reports of the World Health Organization, which focuses on global health issues including access to health care and improving public health outcomes, especially in developing countries.[13] Culture. Gender. Environmental: all matters related to health external to the human body, and over which the individual has little or no control; Lifestyle: the aggregation of personal decisions (i.e. over which the individual has control) that can be said to contribute to, or cause, illness or death; The concept of the health field , as distinct from medical care, emerged from the Lalonde report from Canada. The report identified three interdependent fields as key determinants of an individual s health. These are:[11] Focusing more on lifestyle issues and their relationships with functional health, data from the Alameda County Study suggested that people can improve their health via exercise, enough sleep, maintaining a healthy body weight, limiting alcohol use, and avoiding smoking.[12] The ability to adapt and to self manage have been suggested as core components of human health.[14] Biomedical: all aspects of health, physical and mental, developed within the human body as influenced by genetic make-up. The environment is often cited as an important factor influencing the health status of individuals. This includes characteristics of the natural environment, the built environment, and the social environment. Factors such as clean water and air, adequate housing, and safe communities and roads all have been found to contribute to good health, especially the health of infants and children.[9][15] Some studies have shown that a lack of neighborhood recreational spaces including natural environment leads to lower levels of personal satisfaction and higher levels of obesity, linked to lower overall health and well being.[16] This suggests the positive health benefits of natural space in urban neighborhoods should be taken into account in public policy and land use. Genetics, or inherited traits from parents, also play a role in determining the health status of individuals and populations. This can encompass both the predisposition to certain diseases and health conditions, as well as the habits and behaviors individuals develop through the lifestyle of their families - also referred to as the nature versus nurture debate, in other words the role of factors which can or cannot be controlled. For example, genetics may play a role in the manner in which people cope with stress, either mental, emotional or physical. [edit] Role of science in health. Achieving and maintaining health is an ongoing process, shaped by both the evolution of health care knowledge and practices, as well as personal strategies and organized interventions for staying healthy. [edit] Maintaining health. Health science is the branch of science focused on health. There are two main approaches to health science: the study and research of the body and health-related issues to understand how humans (and animals) function; and the application of that knowledge to improve health and to prevent and cure diseases and other physical and mental impairments. The science builds on many sub fields, including biology, biochemistry, physics, epidemiology, pharmacology, medical sociology, and others. Applied health sciences endeavor to better understand and improve human health through applications in areas such as health education, biomedical engineering, biotechnology and public health. Main articles: Health science and Health care. Organized interventions to improve health based on the principles and procedures developed through the health sciences are delivered among practitioners trained in medicine, nursing, nutrition, pharmacy, social work, psychology, physical therapy and other health care professions. Clinical practitioners focus mainly on the health of individuals, while public health practitioners consider the overall health of communities and populations. Workplace wellness programs are increasingly adopted by companies for their value in improving the health and well-being of their employees, as are school health services to improve the health and well-being of children. [edit] Role of public health. Postage stamp, New Zealand, Public health has been promoted - and depicted - in a wide variety of ways. See also: Global health. Main article: Public health. Public health has been described as the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and private, communities and individuals. [17] It is concerned with threats to the overall health of a community based on population health analysis. The population in question can be as small as a handful of people or as large as all the inhabitants of several continents (for instance, in the case of a pandemic). Public health has many sub-fields, but typically includes the interdisciplinary categories of epidemiology, biostatistics and health services. Environmental health, community health, behavioral health, and occupational health, are also important areas of public health. The focus of public health interventions is to prevent and manage diseases, injuries and other health conditions through surveillance of cases and the promotion of healthy behaviors, communities and environments. Its aim is preventing from happening or re-occurring health problems by implementing educational programs, developing policies, administering services, and conducting research.[18] In many cases, treating a disease or controlling a pathogen can be vital to preventing it in others, such as during an outbreak. Vaccination programs and distribution of condoms to prevent the spread of communicable diseases are examples of common preventive public health measures. Public health also takes several actions to limit the health disparities between different areas of the country, continent or world. The great issue is addressing access of individuals and communities to health care, in terms of financial, geographical or sociocultural constraints in access to and use of services. Applications of the public health system include areas of maternal and child health, health services administration, emergency response, and prevention and control of infectious and chronic diseases. The great positive impact of public health programs is widely acknowledged. Due in part to the policies and actions developed through public health, the 20th century registered a decrease of the mortality rates in infants and children and a continual increase in life expectancy in most parts of the world. For example, it is estimated that the life expectancy has increased for Americans by thirty years since 1900,[19] and worldwide by six years since 1990.[20] See also: Chronic care management, Social relation, and Stress management. Main article: Self care. [edit] Self care strategies. Personal health depends partially on the active, passive, and assisted cues people observe and adopt about their own health. These include personal actions for preventing or minimizing the effects of a disease, usually a chronic condition, through integrative care. They also include personal hygiene practices to prevent infection and illness, such as bathing and washing hands with soap; brushing and flossing teeth; storing, preparing and handling food safely; and many others. The information gleaned from personal observations of daily living - such as about sleep patterns, exercise behavior, nutritional intake, and environmental features - may be used to inform personal decisions and actions (e.g., I feel tired in the morning so I am going to try sleeping on a different pillow ), as well as clinical decisions and treatment plans (e.g., a patient who notices his or her shoes are tighter than usual may be having exacerbation of left-sided heart failure, and may require diuretic medication to reduce fluid overload).[21] Personal health also depends partially on the social structure of a person s life. The maintenance of strong social relationships, volunteering, and other social activities have been linked to positive mental health and even increased longevity. One American study among seniors over age 70 found that frequent volunteering was associated with reduced risk of dying compared with older persons who did not volunteer, regardless of physical health status.[22] Another study from Singapore reported that volunteering retirees had significantly better cognitive performance scores, fewer depressive symptoms, and better mental well-being and life satisfaction than non-volunteering retirees.[23] Prolonged psychological stress may negatively impact health, and has been cited as a factor in cognitive impairment with aging, depressive illness, and expression of disease.[24] Stress management is the application of methods to either reduce stress or increase tolerance to stress. Relaxation techniques are physical methods used to relieve stress. Psychological methods include cognitive therapy, meditation, and positive thinking which work by reducing response to stress. Improving relevant skills, such as problem solving and time management skills, reduces uncertainty and builds confidence, which also reduces the reaction to stress-causing situations where those skills are applicable. complete health information. [edit] See also. Global burden of disease. Book: HealthWikipedia books are collections of articles that can be downloaded or ordered in print.Behavioral change theories. Health and fitness portal. Health care. Health policy. Health education. Health care providers. Primary health care. Health workforce. Health systems. History of medicine. Nutrition. Leveraging Agriculture for Improving Nutrition and Health. Healthy narcissism. ^ Merriam-Webster. Dictionnary - Health , accessed 21 April [edit] References. One Health. ^ World Health Organization [ WHO definition of Health], Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference, New York, 19–22 June 1946; signed on 22 July 1946 by the representatives of 61 States (Official Records of the World Health Organization, no. 2, p. 100) and entered into force on 7 April ^ Jadad AR, O Grady L. How should health be defined BMJ 2008; 337:a ^ Callahan D. The WHO definition of health . The Hastings Center Studies, 1(3), ^ World Health Organization Constitution of the World Health Organization - Basic Documents, Forty-fifth edition, Supplement, October ^ World Health Organization Ottawa Charter for Health Promotion, adopted at the First International Conference on Health Promotion, Ottawa, 21 November WHO/HPR/HEP/95.1. ^ Nutter S The Health Triangle. Anchor Points, Inc. ^ Georgia State University Health Triangle Slides. ^ a b c World Health Organization. The determinants of health. Geneva. Accessed 12 May ^ a b Housman J, Dorman S The Alameda County Study: A Systematic, Chronological Review American Journal of Health Education; 36(5):302–308. ^ a b c Lalonde, Marc. A New Perspective on the Health of Canadians. Ottawa: Minister of Supply and Services; ^ Public Health Agency of Canada. What Determines Health Ottawa. Accessed 12 May ^ UNESCO. The UN World Water Development Report: Facts and Figures - Meeting basic needs. Accessed 12 May ^ Huber M et al. How should we define health BMJ 2011;343 doi: /bmj.d4163 (Published 26 July 2011). Accessed 2 August ^ World Health Organization. The world health report. Geneva. ^ Bjork J et al. Recreational Values of the Natural Environment in Relation to Neighborhood Satisfaction, Physical Activity, Obesity and Well being. J Epidemiol Community Health 2008;62:e2. ^ Association of Schools of Public Health. Impact of Public Health. Retrieved ^ Association of Schools of Public Health. What is Public Health Retrieved ^ C.-E. A. Winslow The Untilled Fields of Public Health, Science, n.s. 51. ^ Harris AHS, Thoresen CE. Volunteering is Associated with Delayed Mortality in Older People: Analysis of the Longitudinal Study of Aging. Journal of Health Psychology, 2005; 10(6): 739–752. ^ Robert Wood Johnson Foundation Health in Everyday Living. ^ World Health Organization. Life expectancy at birth, accessed 20 April ^ Schwingel A et al. Continued work employment and volunteerism and mental well-being of older adults: Singapore longitudinal ageing studies. Age and Ageing, 2009; 38(5): Look up health in Wiktionary, the free dictionary.Wikiquote has a collection of quotations related to: HealthWorld Health and Organization. [edit] External links. ^ McEwen BS (2006). Protective and damaging effects of stress mediators: central role of the brain . Dialogues Clin Neurosci 8 (4): 367–81. PMID OECD Health Statistics. Health On the Net Foundation. UK National Health Service. Health-EU Portal, public health portal of the European Union. Health and Medical Information from the University of Colorado.")
14
1.2 Teoretická východiska Vývoj konceptů zdraví a nemoci
Biomedicínský přístup je založen na zjednodušení, které opomíjí sociální a psychologické aspekty Pozor však na vlastní vývoj poznatků, nelze zjednodušovat, např. vývoj v oblasti duševních nemocí, rozvoj poznání kauzálních vztahů, molekulární medicína Sociální koncepty (sociologie, antropologie, ekonomické aspekty – chudoba, kvalita života, sociální kapitál ) Také zde jsme svědky dynamického vývoje Koncept determinant zdraví Subjektivní vnímání zdraví a nemoci Značné rozdíly ve vztahu ke společenskému postavení, vzdělání, typu osobnosti („riskofil, riskofób“) Na jednotlivé přístupy je nutno pohlížet dynamicky z hlediska jejich vývoje, včetně vzájemného ovlivnění, viz např. oblast duševního zdraví (sociální psychiatrie, biologicky orientovaná psychiatrie, vývoj neurověd, kognitivních věd
 Také zde jsme svědky dynamického vývoje. Koncept determinant zdraví. Subjektivní vnímání zdraví a nemoci. Značné rozdíly ve vztahu ke společenskému postavení, vzdělání, typu osobnosti („riskofil, riskofób ) Na jednotlivé přístupy je nutno pohlížet dynamicky z hlediska jejich vývoje, včetně vzájemného ovlivnění, viz např. oblast duševního zdraví (sociální psychiatrie, biologicky orientovaná psychiatrie, vývoj neurověd, kognitivních věd.")
15
1.4 teoretická východiska Determinanty zdraví a nemoci
Cílem definičního vymezení zdraví je postihnout faktory, které zdraví determinují Naše poznatky o těchto determinantách se postupně vyvíjely poměrně dlouho (několik set let, největšího pokroku bylo dosaženo v posledních 50 letech) V posledních 50 letech jsou shrnuty v konceptu označovaném pojmem DETERMINANTY ZDRAVÍ Kde najdete další informace: Wikipedia: 1.social determinants of health* 2. Knowledge network on social determinants of health 3. Drbal, Kebza, Žáček, Křivohlavý Jump to: navigation, search From Wikipedia, the free encyclopedia Social determinants of health Social determinants of health are the economic and social conditions under which people live which determine their health. They are "societal risk conditions", rather than individual risk factors that either increase or decrease the risk for a disease, for example for cardiovascular disease and type II diabetes. As stated in Social Determinants of Health: The Solid Facts (WHO, 2003): "Health policy was once thought to be about little more than the provision and funding of medical care: the social determinants of health were discussed only among academics. This is now changing. While medical care can prolong survival and improve prognosis after some serious diseases, more important for the health of the population as a whole are the social and economic conditions that make people ill and in need of medical care in the first place. Nevertheless, universal access to medical care is clearly one of the social determinants of health." A succinct statement of what they are and why they are important can be found at Raphael (2008) reinforces this concept: "Social determinants of health are the economic and social conditions that shape the health of individuals, communities, and jurisdictions as a whole. Social determinants of health are the primary determinants of whether individuals stay healthy or become ill (a narrow definition of health). Social determinants of health also determine the extent to which a person possesses the physical, social, and personal resources to identify and achieve personal aspirations, satisfy needs, and cope with the environment (a broader definition of health). Social determinants of health are about the quantity and quality of a variety of resources that a society makes available to its members." p. 2. Contents The definitive Canadian work on the social determinants is the 2009 volume "Social Determinants of Health: Canadian Perspectives" at The definitive work on the social determinants is the 2008 report from the World Health Organisation "Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health at [hide] 3 International Health Inequities 2 Inequalities among Canadians 1 Improving Health Status 4 Cultural and Structuralist Approaches 3.2 Between developing and developed countries 3.1 Between developed countries 5 Neo-materialist approach 8 Public policy 7 Life-course perspective 6 Social comparison approach 11 References 10 See also 9 Politics and political ideology 13 External links 12 Further reading Profound improvements in health status have occurred in industrialized nations such as Canada since It has been hypothesized that access to improved medical care is responsible for these differences, but best estimates are that only 10–15 percent of increased longevity since 1900 in wealthy industrialized nations is due to improved health care.[1] As one illustration, the advent of vaccines and medical treatments are usually held responsible for the profound declines in mortality from infectious diseases in Canada since But by the time vaccines for diseases such as measles, influenza, and polio and treatments for scarlet fever, dramatic declines in mortality had already occurred.[1] [edit] Improving Health Status Improvements in behaviour (e.g., reductions in tobacco use, changes in diet, increased exercise, etc.) have also been hypothesized as responsible for improved longevity, but most analysts conclude that improvements in health are due to the improving material conditions of everyday life experienced by Canadians since 1900.[2][3] These improvements occurred in the areas of early childhood, education, food processing and availability, health and social services, housing, employment security and working conditions and every other social determinant of health. Despite dramatic improvements in health in general, significant inequalities in health among Canadians persist.[4][5][6][7] Access to essential medical procedures is guaranteed by Medicare in Canada. Nevertheless, access to care issues are common[8] and this is particularly the case in regards to required prescription medicines where income is a strong determinant of such access.[9] It is believed however that health care issues account for a relatively small proportion of health status differences that exist among Canadians.[10] As for differences in health behaviours (e.g., tobacco and alcohol use, diet, and physical activity, etc.), studies from as early as the mid 1970s—reinforced by many more studies since then—find their impact upon health to be less important than social determinants of health such as income and other social determinants of health.[11][12][13] [edit] Inequalities among Canadians Instead, evidence indicates that health differences among Canadians result primarily from experiences of qualitatively different living conditions associated with the social determinants of health. As just one example, consider the magnitude of differences in health that are related to the social determinant of health of income. Income is especially important as it serves as a marker of different experiences with many social determinants of health.[14] Income is a determinant of health in itself, but it is also a determinant of the quality of early life, education, employment and working conditions, and food security. Income also is a determinant of the quality of housing, need for a social safety net, the experience of social exclusion, and the experience of unemployment and employment insecurity across the life span. Also, a key aspect of Aboriginal life and the experience of women in Canada is their greater likelihood of living under conditions of low income.[15] In Canada almost a quarter of excess premature years of life lost (mortality prior to age 75) can be attributed to income differences among Canadians.[7] These calculations are obtained by using the mortality in the wealthiest quintile of urban neighbourhoods as a baseline and considering all deaths above that level to be “excess” related to income differences. These analyses indicate that 23% of premature years of life lost to Canadians can be accounted for by differences existing between wealthy and other Canadians.[7] Income is a prime determinant of Canadians’ premature years of life lost and premature mortality from a range of diseases.[16][14] Numerous studies indicate that income levels during early childhood, adolescence, and adulthood are all independent predictors of who develops and eventually succumbs to disease.[17][18][19][20] What are the diseases that differentially kill people of varying income levels? Income-related premature years of life lost can be correlated with death certificate cause of death.[7] Among the not-wealthy, mortality by heart disease and stroke are especially related to income differences. Importantly, premature death by injuries, cancers, infectious disease, and diabetes are also all strongly related to not being wealthy in Canada. These rates are especially high among the least well-off Canadians. In 2002, Statistics Canada examined the predictors of life expectancy, disability-free life expectancy, and the presence of fair or poor health among residents of 136 regions across Canada.[21] The predictors included socio-demographic factors (proportion of Aboriginal population, proportion of visible minority population, unemployment rate, population size, percentage of population aged 65 or over, average income, and average number of years of schooling). Also placed into the analysis were daily smoking rate, obesity rate, infrequent exercise rate, heavy drinking rate, high stress rate, and depression rate. Consistent with most other research, behavioural risk factors were rather weak predictors of health status as compared to socio-economic and demographic measures of which income is a major component.[17][22][23] For life expectancy, the socio-demographic measures predicted 56% of variation (total variation is 100%) among Canadian communities. Daily smoking rate added only 8% more predictive power, obesity rate only another 1%, and exercise rate nothing at all! For disability-free life expectancy, socio-demographics predicted 32% of variation among communities, and daily smoking rated added only another 6% predictive power, obesity rate another 5%, and exercise rate another 3%. Differences among Canadians communities in numbers of residents reporting poor or fair health were related to socio-demographics (25% predictive power) with smoking rate adding 6%, obesity rate adding 10%, and exercise rate adding 3% predictive power. Income-related effects are seen therefore in greater incidence and mortality from just about every affliction that Canadians experience. This is especially the case for chronic diseases. Incidence of, and mortality from, heart disease and stroke, and adult-onset or type 2 diabetes are especially good examples of the importance of the social determinants of health.[24][25] While governments, medical researchers, and public health workers emphasize the importance of traditional adult risk factors (e.g., cholesterol levels, diet, physical activity, and tobacco and alcohol use), it is well established that these are relatively poor predictors of heart disease, stroke, and type 2 diabetes rates among populations.[26][27][28] The factors making a difference are living under conditions of material deprivation as children and adults, stress associated with such conditions, and the adoption of health threatening behaviours as means of coping with these difficult circumstances.[29] In fact, difficult living circumstances during childhood are especially good predictors of these diseases.[30][19][31][32] In addition to predicting adult incidence and death from disease, income differences — and the other social determinants of health related to income — are also related to the health of Canadian children and youth. Canadian children living in low-income families are more likely to experience greater incidence of a variety of illnesses, hospital stays, accidental injuries, mental health problems, lower school achievement and early drop-out, family violence and child abuse, among others.[33] In fact, low-income children show higher incidences of just about any health-, social-, or education-related problem, however defined. These differences in problem incidence occur across the income range but are most concentrated among low-income children.[34][35][36] The traditional 10 Tips for Better Health [37] In one approach the focus is on so-called lifestyle choices. In the other there is a concern with the social determinants of health. 1. Don't smoke. If you can, stop. If you can't, cut down. 4. Manage stress by, for example, talking things through and making time to relax. 3. Keep physically active. 2. Follow a balanced diet with plenty of fruit and vegetables. 5. If you drink alcohol, do so in moderation. 8. Take up cancer-screening opportunities. 7. Practice safer sex. 6. Cover up in the sun, and protect children from sunburn. Ten Tips for Staying Healthy -Gordon, David, 1999 10. Learn the First Aid ABCs: airways, breathing, circulation. 9. Be safe on the roads: follow the Highway Code. 1. Don’t be poor. If you can, stop. If you can’t, try not to be poor for long. 4. Don’t work in a stressful, low paid manual job. 3. Own a car. 2. Don’t have poor parents. 7. Practice not losing your job and don’t become unemployed. 6. Be able to afford to go on a foreign holiday and sunbathe. 5. Don’t live in damp, low quality housing. 8. Take up all benefits you are entitled to, if you are unemployed, retired or sick or disabled. Source: Raphael, D The question of evidence in health promotion. Health Promotion International 15: Table 3, "The role of ideology in health promotion." 10. Learn how to fill in the complex housing benefit/ asylum application forms before you become homeless and destitute. 9. Don’t live next to a busy major road or near a polluting factory. [edit] International Health Inequities Profound differences in overall health status exist between developed and developing nations. Much of this has to do with the lack of the basic necessities of life (food, water, sanitation, primary health care, etc.) common to developing nations. Yet among developed nations such as Canada, less profound but still highly significant differences in health status indicators such as life expectancy, infant mortality, incidence of disease, and death from injuries exist.[38] An excellent example is comparison of health status differences and the hypothesized social determinants of these health status differences among Canada, the United States, and Sweden. [edit] Between developed countries Scholarship has noted that the USA takes an especially laissez-faire approach to providing various forms of security (employment, food, income, and housing) and health and social services while Sweden’s welfare state makes extraordinary efforts to provide security and services.[39][40] The sources of these differences in public policy appear to be in differing commitments to citizen support informed by the political ideologies of governing parties within each nation.[41][42] Emerging scholarship is specifically focused on how national approaches to security provision to citizens influence health by shaping the quality of numerous social determinants of health. Nations such as Sweden whose policies reduce unemployment, minimize income and wealth inequality, and address numerous social determinants of health show evidence of improved population health using indicators such as infant mortality and life expectancy.[43] At the other end, nations with minimal commitments to such efforts such as the United States show rather worse indicators of population health.[44] [edit] Between developing and developed countries Finally, poverty is an especially important indicator of how various social determinants of health combine to influence health. Using child – that is family – poverty rates as an important social determinants of both child and eventual health, Canada does not fare well in relation to European nations. People in rich countries live dramatically longer, healthier lives than people in poorer countries. Thus it can be argued, that it is the huge wealth inequalities between rich and poor countries, that is acting as a fundamental driver of poor global health. The causes of wealth inequalities are discussed elsewhere, and health advocacy groups are forming to lobby for recognition of these issues. To secure attention to the social determinants of health and build support for their strengthening, it is important to understand how social determinants of health come to influence health and cause disease. The very influential UK Black and The Health Divide reports considered two primary mechanisms for understanding this process: cultural/ behavioural and materialist/structuralist.[45] [edit] Cultural and Structuralist Approaches The cultural/behavioural explanation was that individuals' behavioural choices (e.g., tobacco and alcohol use, diet, physical activity, etc.) were responsible for their developing and dying from a variety of diseases. Both the Black and Health divide reports however, showed that behavioural choices are heavily structured by one’s material conditions of life. And—consistent with mounting evidence—these behavioural risk factors account for a relatively small proportion of variation in the incidence and death from various diseases. The materialist/structuralist explanation emphasizes the material conditions under which people live their lives. These conditions include availability of resources to access the amenities of life, working conditions, and quality of available food and housing among others. The author of the Health Divide concluded: The weight of evidence continues to point to explanations which suggest that socio-economic circumstances play the major part in subsequent health differences.[46] Despite this conclusion and increasing evidence in favour of this view, much of the Canadian public discourse on health and disease remains focused on “life-style” approaches to disease prevention.[47] These materialist/structuralist conceptualizations have been refined such that analysis is now focused upon three frameworks by which social determinants of health come to influence health.[48] These frameworks are: (a) materialist; (b) neo-materialist; and (c) psychosocial comparison. The materialist explanation is about how living conditions – and the social determinants of health that constitute these living conditions—shape health. The neo-materialist explanation extends the materialist analysis by asking how these living conditions come about. The psychosocial comparison explanation considers whether people compare themselves to others and how these comparisons affect health and wellbeing. In this argument individuals experience varying degrees of positive and negative exposures over their lives that accumulate to produce adult health outcomes.[49] Overall wealth of nations is a strong indicator of population health. But within nations, socio-economic position is a powerful predictor of health as it is an indicator of material advantage or disadvantage over the lifespan.[50] Material conditions of life determine health by influencing the quality of individual development, family life and interaction, and community environments. Material conditions of life lead to differing likelihood of physical (infections, malnutrition, chronic disease, and injuries), developmental (delayed or impaired cognitive, personality, and social development), educational (learning disabilities, poor learning, early school leaving), and social (socialization, preparation for work, and family life) problems.[44][49] Material conditions of life also lead to differences in psychosocial stress[51] The fight-or-flight reaction—chronically elicited in response to threats such as income, housing, and food insecurity, among others—weakens the immune system, leads to increased insulin resistance, greater incidence of lipid and clotting disorders, and other biomedical insults that are precursors to adult disease. Adoption of health-threatening behaviours is a response to material deprivation and stress.[52] Environments determine whether individuals take up tobacco, use alcohol, experience poor diets, and have low levels of physical activity. Tobacco and excessive alcohol use, and carbohydrate-dense diets are also means of coping with difficult circumstances.[53][54] Materialist arguments help us understand the sources of health inequalities among individuals and nations and the role played by the social determinants of health. [edit] Neo-materialist approach Exposures to the material conditions of life are important for health, but why are these material conditions so unequally distributed among the Canadian population but less so elsewhere?.[55][56] The neo-materialist approach is concerned with how nations, regions, and cities differ on how economic and other resources are distributed among the population.[57] Some jurisdictions have more equalitarian distribution of resources such that there are fewer poor people and the gaps that exist among the population in their exposures to the social determinants of health is narrower than places where there are more poor people and the gaps among the population are greater. In the USA, states and cities with more unequal distributions of income have more low-income people and greater income gaps between rich and poor. They invest less in public infrastructure such as education, health and social services, health insurance, supports for the unemployed and those with disabilities, and spend less on education and libraries. All of these issues contribute to the quality of the social determinants of health to which people are exposed. Such unequal jurisdictions have much poorer health profiles than more equalitarian places.[58][59] Canada has a smaller proportion of lower-income people, a smaller gap between rich and poor, and spends relatively more on public infrastructure than the U.S.[60] Not surprisingly, Canadians enjoy better health than Americans as measured by infant mortality rates, life expectancy, and death rates from childhood injuries.[10] Neither nation does as well as Sweden where distribution of resources is much more equalitarian, low-income rates are very low, and health indicators are among the best in the world. The neo-materialist view therefore, directs attention to both the effects of living conditions – the social determinants of health—on individuals' health and the societal factors that determine the quality of the distribution of these social determinants of health. How a society decides to distribute resources among citizens is especially important. [edit] Social comparison approach At the individual level, the perception and experience of one’s status in unequal societies lead to stress and poor health. Comparing their status, possessions, and other life circumstances to those better-off than themselves, individuals experience feelings of shame, worthlessness, and envy that have psychobiological effects upon health. These processes involve direct disease-producing effects upon neuro-endocrine, autonomic and metabolic, and immune systems.[51] These comparisons can also lead to attempts to alleviate such feelings by overspending, taking on additional employment that threaten health, and adopting health-threatening coping behaviours such as overeating and using alcohol and tobacco.[61] The argument here is that the social determinants of health play their role through citizens’ interpretations of their standings in the social hierarchy.[61][56] There are two mechanisms by which this occurs. At the communal level, widening and strengthening of hierarchy weakens social cohesion, a determinant of health.[62] Individuals become more distrusting and suspicious of others with direct stress-related effects on the body. Such attitudes can also weaken support for communal structures such as public education, health, and social programs. An exaggerated desire for tax reductions on the part of the public can weaken public infrastructure. This approach directs attention to the psychosocial effects of public policies that weaken the social determinants of health. But these effects may be secondary to how societies distribute material resources and provide security to its citizens – processes described in the materialist and neo-materialist approaches. Material aspects may be paramount and the stresses associated with deprivation simply add to the toll on individuals’ bodies. Traditional approaches to health and disease prevention have a distinctly non-historical here-and-now emphasis. Usually adults, and increasingly adolescents and youth are urged to adopt “healthy lifestyles” as a means of preventing the development of chronic diseases such as heart disease and diabetes, among others.[63][64] In contrast to these approaches, life-course approaches emphasize the accumulated effects of experience across the life span in understanding the maintenance of health and the onset of disease. It has been argued: [edit] Life-course perspective “The prevailing aetiological model for adult disease which emphasizes adult risk factors, particularly aspects of adult life style, has been challenged in recent years by research that has shown that poor growth and development and adverse early environmental conditions are associated with an increased risk of adult chronic disease" Kuh, D., & Ben-Shilmo, Y. (Eds.). (1997). A life course approach to chronic disease epidemiology. Oxford, UK: Oxford University Press,p.3. More specifically, it is apparent that the economic and social conditions—the social determinants of health—under which individuals live their lives have a cumulative effect upon the probability of developing any number of diseases. This has been repeatedly demonstrated in longitudinal studies—the U.S. National Longitudinal Survey, the West of Scotland Collaborative Study, Norwegian and Finnish linked data—which follow individuals across their lives.[65] This has been most clearly demonstrated in the case of heart disease and stroke.[25] And most recently, studies into the childhood and adulthood antecedents of adult-onset diabetes show how adverse economic and social conditions across the life span predispose individuals to this disorder.[28][66][40] A recent volume brings together some of the important work concerning the importance of a life-course perspective for understanding the importance of social determinants.[67] Adopting a life-course perspective directs attention to how social determinants of health operate at every level of development—early childhood, childhood, adolescence, and adulthood—to both immediately influence health as well as provide the basis for health or illness during later stages of the life course. Hertzman outlines three health effects that have relevance for a life-course perspective.[68] Latent effects are biological or developmental early life experiences that influence health later in life. Low birth weight, for instance, is a reliable predictor of incidence of cardiovascular disease and adult-onset diabetes in later life. Experience of nutritional deprivation during childhood has lasting health effects. Pathway effects are experiences that set individuals onto trajectories that influence health, well-being, and competence over the life course. As one example, children who enter school with delayed vocabulary are set upon a path that leads to lower educational expectations, poor employment prospects, and greater likelihood of illness and disease across the lifespan. Deprivation associated with poor-quality neighbourhoods, schools, and housing sets children off on paths that are not conducive to health and well-being. Cumulative effects are the accumulation of advantage or disadvantage over time that manifests itself in poor health. These involve the combination of latent and pathways effects. Adopting a life-course perspective directs attention to how social determinants of health operate at every level of development—early childhood, childhood, adolescence, and adulthood—to both immediately influence health and provide the basis for health or illness later in life. Much social determinants of health research simply focuses on determining the relationship between a social determinant of health and health status. So a researcher may document that lower income is associated with adverse health outcomes among parents and their children. Or a researcher may demonstrate that food insecurity is related to poor health status among parents and children as is living in crowded housing, and so on. This is what is termed a depoliticized approach in that it says little about how these poor-quality social determinants of health come about.[69] [edit] Public policy Social determinants of health do not exist in a vacuum. Their quality and availability to the population are usually a result of public policy decisions made by governing authorities. As one example, consider the social determinant of health of early life. Early life is shaped by availability of sufficient material resources that assure adequate educational opportunities, food and housing among others. Much of this has to do with the employment security and the quality of working conditions and wages. The availability of quality, regulated childcare is an especially important policy option in support of early life. [70] These are not issues that usually come under individual control. A policy-oriented approach places such findings within a broader policy context. Yet it is not uncommon to see governmental and other authorities individualize these issues. Governments may choose to understand early life as being primarily about parental behaviours towards their children. They then focus upon promoting better parenting, assist in having parents read to their children, or urge schools to foster exercise among children rather than raising the amount of financial or housing resources available to families. Indeed, for every social determinant of health, an individualized manifestation of each is available. There is little evidence to suggest the efficacy of such approaches in improving the health status of those most vulnerable to illness in the absence of efforts to modify their adverse living conditions.[71] One way to think about this is to consider the idea of the welfare state and the political ideologies that shape its form in Canada and elsewhere. The concept of the welfare state is about the extent to which governments – or the state – use their power to provide citizens with the means to live secure and satisfying lives. Every developed nation has some form of the welfare state. [edit] Politics and political ideology Two literature's inform this analysis. The first concerns the three forms of the modern welfare state. Esping-Andersen identifies three distinct clusters of welfare regimes among wealthy developed nations: Social Democratic (e.g., Sweden, Norway, Denmark, and Finland), Liberal (USA, UK, Canada, Ireland), and Conservative (France, Germany, Netherlands, and Belgium, among others).[72][73] There is high government intervention and strong welfare systems in the social democratic countries and rather less in the liberal. Conservative nations fall midway between these others in service provision and citizen supports. Social democratic nations have very well developed welfare states that provide a wide range of universal and generous benefits. They expend more of national wealth to supports and services. They are proactive in developing labour, family-friendly, and gender equity supporting policies. Liberal nations spend rather less on supports and services. They offer modest universal transfers and modest social-insurance plans. Benefits are provided primarily through means-tested assistance whereby these benefits are only provided to the least well-off. Navarro and colleagues provide empirical support for the hypotheses that the social determinants of health and health status outcomes are of higher quality in the social democratic rather than the liberal nations.[74][42] Some of these indicators are spending on supports and services, equitable distribution of income, and wealth and availability of services in support of families and individuals. Health indicators include life expectancy and infant mortality. A particularly important issue that is emerging is whether any particular analysis of social determinants of health is de-politicized or not. A de-politicized approach is one that fails to take account of the fact that the quality of the social determinants of health to which citizens in a jurisdiction are exposed to is shaped by public policy created by governments. And governments of course are controlled by political parties who come to power with a set of ideological beliefs concerning the nature of society and the role of governments. Could this general approach to welfare provision shape Canadian receptivity to the concepts developed in this volume? And if so, what can be done to improve receptivity to and implementation of these concepts? The final chapter of this volume revisits these issues. Such analyses that recognize the role played by politics outline the particular importance of having social democratic political parties in power. Nations that have had longer periods of social democratic influence such as Norway, Finland, Sweden, and Denmark have government policymaking that is remarkably consistent with social determinants of health concepts. Nations such as the USA and Canada,dominated by liberal and neo-liberal governing parties, much less so. The weight of the evidence suggests that the SDOH have a direct impact on the health of individuals and populations, are the best predictors of individual and population health, structure lifestyle choices, and interact with each other to produce health (Raphael, 2003). In terms of the health of populations, it is well known that disparities-the size of the gap or inequality in social and economic status between groups within a given population-greatly affect the health status of the whole. The larger the gap, the lower the health status of the overall population.[53][54] An example of SDOH, applicable to the United States, is shown in the graph. It shows self-reported health as it relates to income level and political party identification (Democrat vs. Republican).[77] A wealth of evidence from Canada and other countries supports the notion that the socioeconomic circumstances of individuals and groups are equally or more important to health status than medical care and personal health behaviours, such as smoking and eating patterns. [75][76] Health literacy Health equity [edit] See also Global health Population health Diseases of poverty Diseases of affluence Whitehall Study Hopkins Center for Health Disparities Solutions Population Health Forum Center for Minority Health Social epidemiology Social determinants of obesity Race and health Medical sociology Medical anthropology Unnatural Causes: Is Inequality Making Us Sick? Michael Marmot [edit] References Dennis Raphael Richard G. Wilkinson ^ McKeown, T., & Record, R. G. (1975). An interpretation of the decline in mortality in England and Wales during the twentieth century. Population Studies, 29, ^ McKeown, T. (1976). The Role of Medicine: Dream, Mirage, or Nemesis. London UK: Neufeld Provincial Hospitals Trust. ^ a b McKinlay, J., & McKinlay, S. M. (1987). Medical measures and the decline of mortality. In H. D. Schwartz (Ed.), Dominant issues in medical sociology (2nd edition ed.). New York: Random House. ^ Canadian Population Health Initiative. (2004). Improving the Health of Canadians. Ottawa: CPHI. ^ a b c d Wilkins, R., Berthelot, J.-M., & Ng, E. (2002). Trends in mortality by neighbourhood income in urban Canada from 1971 to Health Reports (Stats Can), 13(Supplement), 1-28. ^ Health Canada. (1999). Toward a Healthy Future: Second Report on the Health of Canadians. Retrieved August, 2002, from ^ Canadian Population Health Initiative. (2008). Reducing Gaps in Health: A Focus on Socio-Economic Status in Urban Canada. Ottawa: Canadian Population Health Initiative. ^ a b Siddiqi, A., & Hertzman, C. (2007). Towards an epidemiological understanding of the effects of long-term institutional changes on population health: A case study of Canada versus the USA. Social Science & Medicine, 64(3), ^ Raphael, D. (2007). Interactions with the health and service sector. In D. Raphael (Ed.), Poverty and policy in Canada: Implications for health and quality of life. (pp ). Toronto: Canadian Scholars' Press. ^ McGibbon, E. (2008). Health and health care: A human rights perspective. In D. Raphael (Ed.), Social Determinants of Health: Canadian Perspectives (2nd ed., pp ). Toronto: Canadian Scholars' Press. ^ Marmot, M., Shipley, M., Brunner, E., & Hemingway, H. (2001). Relative Contribution of Early Life and Adult Socioeconomic Factors to Adult Morbidity in the Whitehall II Study. Journal of Epidemiology and Community Health, 2001(55), 5. ^ a b Raphael, D., Macdonald, J., Labonte, R., Colman, R., Hayward, K., & Torgerson, R. (2004). Researching income and income distribution as a determinant of health in Canada: Gaps between theoretical knowledge, research practice, and policy implementation. Health Policy, 72, ^ Raphael, D. (2007). Poverty and Health: Mechanisms and Pathways. In D. Raphael (Ed.), Poverty and Policy in Canada: Implications for Health and Quality of Life (pp ). Toronto: Canadian Scholars' Press. ^ Nettleton, S. (1997). Surveillance, health promotion and the formation of a risk identity. In M. Sidell, L. Jones, J. Katz & A. Peberdy (Eds.), Debates and Dilemmas in Promoting Health (pp ). London, UK: Open University Press. ^ a b Benzeval, M., Dilnot, A., Judge, K., & Taylor, J. (2001). Income and health over the lifecourse: Evidence and policy implications. In H. Graham (Ed.), Understanding Health Inequalities (pp ). Buckingham, UK: Open University Press. ^ Raphael, D., Labonte, R., Colman, R., Torgeson, R., Hayward, K., & Macdonald, J. (2006). Income and health research in Canada: Needs, gaps, and opportunities. Canadian Journal of Public Health, 97(Supplement #3), s16-s23. ^ Raphael, D. (2007). Who is poor in Canada? In D. Raphael (Ed.), Poverty and policy in Canada: Implications for health and quality of life, (pp ). Toronto: Canadian Scholars' Press. ^ Benzeval, M., & Judge, K. (2001). Income and health: The time dimension. Social Science & Medicine, 52, ^ Shields, M., & Tremblay, S. (2002). The Health of Canada's Communities. Health Reports. Supplement, 13(July), 1-22. ^ Judge, K., & Paterson, I. (2002). Treasury Working Paper: Poverty, Income Inequality and Health. Wellington, NZ: Government of New Zealand. ^ a b Davey Smith, G., & Hart, C. (2002). Life-Course Approaches to Socio-Economic and Behavioural Influences on Cardiovascular Disease Mortality. American Journal of Public Health, 92(8), ^ Raphael, D., Anstice, S., & Raine, K. (2003). The social determinants of the incidence and management of Type 2 Diabetes Mellitus: Are we prepared to rethink our questions and redirect our research activities? Leadership in Health Services, 16, 10-20 ^ Roux, A., Merkin, S., & Arnett, D. (2001). Neighbourhood of Residence and Incidence of Coronary Heart Disease. New England Journal of Medicine, 345, ^ Lantz, P. M., House, J. S., Lepkowski, J. M., Williams, D. R., Mero, R. P., & Chen, J. J. (1998). Socioeconomic factors, health behaviors, and mortality. Journal of the American Medical Association, 279(21), ^ a b Raphael, D., & Farrell, E. S. (2002). Beyond medicine and lifestyle: Addressing the societal determinants of cardiovascular disease in North America. Leadership in Health Services, 15, 1-5. ^ a b Lawlor, D., Ebrahim, S., & Smith, G. D. (2002). Socioeconomic position in childhood and adulthood and insulin resistance: cross sectional survey using data from British women's heart and health study. British Medical Journal, 325(12), ^ Davey Smith, G., Ben-Shlomo, Y., & Lynch, J. (2002). Life course approaches to inequalities in coronary heart disease risk. In S. A. Stansfeld & M. Marmot (Eds.), Stress and the Heart: Psychosocial Pathways to Coronary Heart Disease (pp ). London, UK: BMJ Books. ^ Chaufan, C. (2008). What does justice have to do with it? A bioethical and sociological perspective on the diabetes epidemic. Bioethical Issues, Sociological Perspectives, 9, ^ Eriksson, J., Forsen, T., Tuomilehto, J., Winter, P., Osmond, C., & Barker, D. (1999). Catch-up growth in childhood and death from coronary heart disease: longitudinal study. BMJ - Clinical Research, 318(7181), ^ Barker, D. J., Osmond, C., & Simmonds, M. (1989). Weight in infancy and death from ischemic heart disease. The Lancet, 2, ^ Benzeval, M., Judge, K., & Whitehead, M. (1995). Tackling Inequalities in Health: An Agenda for Action. London: Kings Fund. ^ Eriksson, J. G., Forsen, T., Tuomilehto, J., Osmond, C., & Barker, B. J. (2001). Early Growth and Coronary Heart Disease in later life: Longitudinal Study. British Medical Journal, 322, ^ Ross, D. P., Roberts, P., & Scott, K. (2000). Family income and child well-being. ISUMA, 1(2), ^ Ross, D. P., & Roberts, P. (1999). Income and Child Well-Being: A New Perspective on the Poverty Debate. Ottawa, Canada: Canadian Council on Social Development. ^ Canadian Institute on Children's Health. (2000). The Health of Canada's Children: A CICH Profile 3rd Edition. Ottawa, Canada: Canadian Institute on Children's Health. ^ Organisation for Economic Cooperation and Development. (2007). Health at a Glance 2007, OECD Indicators. Paris: Organisation for Economic Cooperation and Development. ^ L. Donaldson, Ten Tips for Better Health (London: Stationary Office, 1999). ^ Willms, J. D. (Ed.). (2002). Vulnerable Children: Findings from Canada's National Longitudinal Survey. Edmonton, AB: University of Alberta Press. ^ Burstrom, B., Diderichsen, F., Ostlin, P., & Ostergren, P. O. (2002). Sweden. In J. Mackenbach & M. Bakker (Eds.), Reducing Inequalities in Health: A European Perspective (pp ). London UK: Routledge. ^ a b Navarro, V., & Shi, L. (2002). The political context of social inequalities and health. In V. Navarro (Ed.), The Political Economy of Social Inequalities: Consequences for Health and Quality of Life (pp ). Amityville, NY: Baywood. ^ Bambra, C. (2004). The worlds of welfare: illusory and gender blind? Social Policy and Society, 3(3), ^ a b Raphael, D., & Bryant, T. (2006). The State's role in promoting population health: Public health concerns in Canada, USA, UK, and Sweden. Health Policy, 78, ^ Townsend, P., Davidson, N., & Whitehead, M. (Eds.). (1992). Inequalities in Health: the Black Report and the Health Divide. New York: Penguin. ^ a b Raphael, D. (2007c). Poverty and Health. In D. Raphael (Ed.), Poverty and Policy in Canada: Implications for Health and Quality of Life (pp ). Toronto: Canadian Scholars' Press. ^ Diderichsen, F., Whitehead, M., Burstrom, B., & Aberg, M. (2001). Sweden and Britain: The impact of policy context on inequities in health. In T. Evans, M. Whitehead, F. Diderichsen, A. Bhuya & M. Wirth (Eds.), Challenging Inequities in Health: from Ethics to Action (pp ). New York: Oxford University Press. ^ Whitehead, M. (1992). The health divide. In P. Townsend, N. Davidson & M. Whitehead (Eds.), Inequalities in Health: the Black Report and the Health Divide (pp ). New York: Penguin. ^ a b Shaw, M., Dorling, D., Gordon, D., & Smith, G. D. (1999). The Widening Gap: Health Inequalities and Policy in Britain. Bristol, UK: The Policy Press. ^ Bartley, M. (2003). Understanding Health Inequalities. Oxford UK: Polity Press. ^ Raphael, D. (2008a). Grasping at straws: A recent history of health promotion in Canada. Critical Public Health, 18(4), ^ Jarvis, M. J., & Wardle, J. (2003). Social patterning of individual health behaviours: the case of cigarette smoking. In M. G. ^ a b Brunner, E., & Marmot, M. G. (2006). Social organization, stress, and health. In M. G. Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp. 6-30). Oxford: Oxford University Press. ^ Graham, H. (2007). Unequal Lives: Health and Socioeconomic Inequalities. New York: Open University Press. ^ a b Wilkinson, R. G. (1996). Unhealthy Societies: The Afflictions of Inequality. New York: Routledge. ^ a b Tarlov, A. (1996). Social determinants of health: The sociobiological translation. In D. Blane, E. Brunner & R. Wilkinson (Eds.), Health and Social Organization: Towards a Health Policy for the 21st Century (pp ). London UK: Routledge. ^ Graham, H. (2004). Social determinants and their unequal distribution: Clarifying policy understandings. Milbank Quarterly, 82(1), ^ a b Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp ). Oxford, UK: Oxford University Press. ^ Lynch, J. W., Kaplan, G. A., Pamuk, E. R., Cohen, R., Heck, C., Balfour, J., et al. (1998). Income inequality and mortality in metropolitan areas of the United States. American Journal of Public Health, 88, ^ Kaplan, G. A., Pamuk, E. R., Lynch, J. W., Cohen, J. W., & Balfour, J. L. (1996). Income Inequality and Mortality in The United States. BMJ, 312, ^ Lynch, J. W., Smith, G. D., Kaplan, G. A., & House, J. S. (2000). Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ, 320, ^ Ross, N., Wolfson, M., Dunn, J., Berthelot, J. M., Kaplan, G., & Lynch, J. (2000). Relation between income inequality and mortality in Canada and in the United States: Cross sectional assessment using census data and vital statistics. BMJ, 320(7239), ^ Chronic Disease Prevention Alliance of Canada. (2003). Who We Are. Retrieved April 16, 2003, from ^ Kawachi, I., & Kennedy, B. P. (1997). Socioeconomic determinants of health : Health and social cohesion: why care about income inequality? BMJ, 314(7086), ^ a b Kawachi, I., & Kennedy, B. (2002). The Health of Nations: Why Inequality Is Harmful to Your Health. New York: New Press. ^ Raphael, D., Anstice, S., & Raine, K. (2003). The social determinants of the incidence and management of Type 2 Diabetes Mellitus: Are we prepared to rethink our questions and redirect our research activities? Leadership in Health Services, 16, ^ Blane, D. (2006). The life course, the social gradiant and health. In M. G. Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp ). Oxford: Oxford University Press. ^ Health Canada. (2003). Healthy Living Strategy. Retrieved April 16, 2003, from ^ Davey Smith, G. (Ed.). (2003). Inequalities in Health: Life Course Perspectives. Bristol UK: Policy Press. ^ Esping-Andersen, G. (2002). A child-centred social investment strategy. In G. Esping-Andersen (Ed.), Why we need a new welfare state (pp ). Oxford UK: Oxford University Press. ^ Raphael, D., & Bryant, T. (2002). The limitations of population health as a model for a new public health. Health Promotion International, 17, ^ Hertzman, C. (2000). The case for an early childhood development strategy. Isuma, Autumn. ^ Esping-Andersen, G. (1999). Social Foundations of Post-Industrial Economies. New York: Oxford University Press. ^ Esping-Andersen, G. (1990). The Three Worlds of Welfare Capitalism. Princeton: Princeton University Press. ^ Raphael, D. (2001). Inequality is Bad for our Hearts: Why Low Income and Social Exclusion are Major Causes of Heart Disease in Canada, from ^ Navarro, V. (Ed.). (2004). The Political and Social Contexts of Health. Amityville NY: Baywood Press. ^ Fried, Joseph, Democrats and Republicans - Rhetoric and Reality (New York: Algora Publishing, 2008), 25. ^ Restrepo, H. E. (2000). Health Promotion: An Anthology. In H. E. Restrepo (Ed.), (pp. ix-xi). Washington, DC: Pan American Health Organization ^ Evans, R. G., Barer, M. L., & Marmor, T. R. (1994). Why Are Some People Healthy and Others Not?: The Determinants of Health of Populations. New York: Aldine de Gruyter. Health Canada. (2001). The Population Health Template: Key Elements and Actions That Define A Population Health Approach. Retrieved June, 2002, from Raphael, D. (2010). About Canada: Health and Illness, Retrieved August, 2010, from [edit] Further reading Raphael, D. (2008c). Public policy and population health in the USA: Why is the public health community missing in action? International Journal of Health Services, 38, Social Determinants of Health: The Canadian Facts [edit] External links Social Determinants of Health: Canadian Perspectives provides the latest developments and is available at Excerpts are available at About Canada: Health and Illness Population Health Forum website World Health Organization: Commission on Social Determinants of Health Public Health Agency of Canada: What determines health? - Key Determinants CBC Ideas - Sick People or Sick Societies? Part 1 and Part 2 VIDEO: Health Status Disparities in the US featuring Paula Braveman, Gregg Bloche, George Kaplan, Thomas Ricketts, Mary Lou deLeon Siantz, and David Williams
 V posledních 50 letech jsou shrnuty v konceptu označovaném pojmem DETERMINANTY ZDRAVÍ. Kde najdete další informace: Wikipedia: 1.social determinants of health* 2. Knowledge network on social determinants of health. 3. Drbal, Kebza, Žáček, Křivohlavý. Jump to: navigation, search. From Wikipedia, the free encyclopedia. Social determinants of health. Social determinants of health are the economic and social conditions under which people live which determine their health. They are societal risk conditions , rather than individual risk factors that either increase or decrease the risk for a disease, for example for cardiovascular disease and type II diabetes. As stated in Social Determinants of Health: The Solid Facts (WHO, 2003): Health policy was once thought to be about little more than the provision and funding of medical care: the social determinants of health were discussed only among academics. This is now changing. While medical care can prolong survival and improve prognosis after some serious diseases, more important for the health of the population as a whole are the social and economic conditions that make people ill and in need of medical care in the first place. Nevertheless, universal access to medical care is clearly one of the social determinants of health. A succinct statement of what they are and why they are important can be found at Raphael (2008) reinforces this concept: Social determinants of health are the economic and social conditions that shape the health of individuals, communities, and jurisdictions as a whole. Social determinants of health are the primary determinants of whether individuals stay healthy or become ill (a narrow definition of health). Social determinants of health also determine the extent to which a person possesses the physical, social, and personal resources to identify and achieve personal aspirations, satisfy needs, and cope with the environment (a broader definition of health). Social determinants of health are about the quantity and quality of a variety of resources that a society makes available to its members. p. 2. Contents. The definitive Canadian work on the social determinants is the 2009 volume Social Determinants of Health: Canadian Perspectives at The definitive work on the social determinants is the 2008 report from the World Health Organisation Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health at [hide] 3 International Health Inequities. 2 Inequalities among Canadians. 1 Improving Health Status. 4 Cultural and Structuralist Approaches. 3.2 Between developing and developed countries. 3.1 Between developed countries. 5 Neo-materialist approach. 8 Public policy. 7 Life-course perspective. 6 Social comparison approach. 11 References. 10 See also. 9 Politics and political ideology. 13 External links. 12 Further reading. Profound improvements in health status have occurred in industrialized nations such as Canada since It has been hypothesized that access to improved medical care is responsible for these differences, but best estimates are that only 10–15 percent of increased longevity since 1900 in wealthy industrialized nations is due to improved health care.[1] As one illustration, the advent of vaccines and medical treatments are usually held responsible for the profound declines in mortality from infectious diseases in Canada since But by the time vaccines for diseases such as measles, influenza, and polio and treatments for scarlet fever, dramatic declines in mortality had already occurred.[1] [edit] Improving Health Status. Improvements in behaviour (e.g., reductions in tobacco use, changes in diet, increased exercise, etc.) have also been hypothesized as responsible for improved longevity, but most analysts conclude that improvements in health are due to the improving material conditions of everyday life experienced by Canadians since 1900.[2][3] These improvements occurred in the areas of early childhood, education, food processing and availability, health and social services, housing, employment security and working conditions and every other social determinant of health. Despite dramatic improvements in health in general, significant inequalities in health among Canadians persist.[4][5][6][7] Access to essential medical procedures is guaranteed by Medicare in Canada. Nevertheless, access to care issues are common[8] and this is particularly the case in regards to required prescription medicines where income is a strong determinant of such access.[9] It is believed however that health care issues account for a relatively small proportion of health status differences that exist among Canadians.[10] As for differences in health behaviours (e.g., tobacco and alcohol use, diet, and physical activity, etc.), studies from as early as the mid 1970s—reinforced by many more studies since then—find their impact upon health to be less important than social determinants of health such as income and other social determinants of health.[11][12][13] [edit] Inequalities among Canadians. Instead, evidence indicates that health differences among Canadians result primarily from experiences of qualitatively different living conditions associated with the social determinants of health. As just one example, consider the magnitude of differences in health that are related to the social determinant of health of income. Income is especially important as it serves as a marker of different experiences with many social determinants of health.[14] Income is a determinant of health in itself, but it is also a determinant of the quality of early life, education, employment and working conditions, and food security. Income also is a determinant of the quality of housing, need for a social safety net, the experience of social exclusion, and the experience of unemployment and employment insecurity across the life span. Also, a key aspect of Aboriginal life and the experience of women in Canada is their greater likelihood of living under conditions of low income.[15] In Canada almost a quarter of excess premature years of life lost (mortality prior to age 75) can be attributed to income differences among Canadians.[7] These calculations are obtained by using the mortality in the wealthiest quintile of urban neighbourhoods as a baseline and considering all deaths above that level to be excess related to income differences. These analyses indicate that 23% of premature years of life lost to Canadians can be accounted for by differences existing between wealthy and other Canadians.[7] Income is a prime determinant of Canadians’ premature years of life lost and premature mortality from a range of diseases.[16][14] Numerous studies indicate that income levels during early childhood, adolescence, and adulthood are all independent predictors of who develops and eventually succumbs to disease.[17][18][19][20] What are the diseases that differentially kill people of varying income levels Income-related premature years of life lost can be correlated with death certificate cause of death.[7] Among the not-wealthy, mortality by heart disease and stroke are especially related to income differences. Importantly, premature death by injuries, cancers, infectious disease, and diabetes are also all strongly related to not being wealthy in Canada. These rates are especially high among the least well-off Canadians. In 2002, Statistics Canada examined the predictors of life expectancy, disability-free life expectancy, and the presence of fair or poor health among residents of 136 regions across Canada.[21] The predictors included socio-demographic factors (proportion of Aboriginal population, proportion of visible minority population, unemployment rate, population size, percentage of population aged 65 or over, average income, and average number of years of schooling). Also placed into the analysis were daily smoking rate, obesity rate, infrequent exercise rate, heavy drinking rate, high stress rate, and depression rate. Consistent with most other research, behavioural risk factors were rather weak predictors of health status as compared to socio-economic and demographic measures of which income is a major component.[17][22][23] For life expectancy, the socio-demographic measures predicted 56% of variation (total variation is 100%) among Canadian communities. Daily smoking rate added only 8% more predictive power, obesity rate only another 1%, and exercise rate nothing at all! For disability-free life expectancy, socio-demographics predicted 32% of variation among communities, and daily smoking rated added only another 6% predictive power, obesity rate another 5%, and exercise rate another 3%. Differences among Canadians communities in numbers of residents reporting poor or fair health were related to socio-demographics (25% predictive power) with smoking rate adding 6%, obesity rate adding 10%, and exercise rate adding 3% predictive power. Income-related effects are seen therefore in greater incidence and mortality from just about every affliction that Canadians experience. This is especially the case for chronic diseases. Incidence of, and mortality from, heart disease and stroke, and adult-onset or type 2 diabetes are especially good examples of the importance of the social determinants of health.[24][25] While governments, medical researchers, and public health workers emphasize the importance of traditional adult risk factors (e.g., cholesterol levels, diet, physical activity, and tobacco and alcohol use), it is well established that these are relatively poor predictors of heart disease, stroke, and type 2 diabetes rates among populations.[26][27][28] The factors making a difference are living under conditions of material deprivation as children and adults, stress associated with such conditions, and the adoption of health threatening behaviours as means of coping with these difficult circumstances.[29] In fact, difficult living circumstances during childhood are especially good predictors of these diseases.[30][19][31][32] In addition to predicting adult incidence and death from disease, income differences — and the other social determinants of health related to income — are also related to the health of Canadian children and youth. Canadian children living in low-income families are more likely to experience greater incidence of a variety of illnesses, hospital stays, accidental injuries, mental health problems, lower school achievement and early drop-out, family violence and child abuse, among others.[33] In fact, low-income children show higher incidences of just about any health-, social-, or education-related problem, however defined. These differences in problem incidence occur across the income range but are most concentrated among low-income children.[34][35][36] The traditional 10 Tips for Better Health [37] In one approach the focus is on so-called lifestyle choices. In the other there is a concern with the social determinants of health. 1. Don t smoke. If you can, stop. If you can t, cut down. 4. Manage stress by, for example, talking things through and making time to relax. 3. Keep physically active. 2. Follow a balanced diet with plenty of fruit and vegetables. 5. If you drink alcohol, do so in moderation. 8. Take up cancer-screening opportunities. 7. Practice safer sex. 6. Cover up in the sun, and protect children from sunburn. Ten Tips for Staying Healthy -Gordon, David, Learn the First Aid ABCs: airways, breathing, circulation. 9. Be safe on the roads: follow the Highway Code. 1. Don’t be poor. If you can, stop. If you can’t, try not to be poor for long. 4. Don’t work in a stressful, low paid manual job. 3. Own a car. 2. Don’t have poor parents. 7. Practice not losing your job and don’t become unemployed. 6. Be able to afford to go on a foreign holiday and sunbathe. 5. Don’t live in damp, low quality housing. 8. Take up all benefits you are entitled to, if you are unemployed, retired or sick or disabled. Source: Raphael, D The question of evidence in health promotion. Health Promotion International 15: Table 3, The role of ideology in health promotion. 10. Learn how to fill in the complex housing benefit/ asylum application forms before you become homeless and destitute. 9. Don’t live next to a busy major road or near a polluting factory. [edit] International Health Inequities. Profound differences in overall health status exist between developed and developing nations. Much of this has to do with the lack of the basic necessities of life (food, water, sanitation, primary health care, etc.) common to developing nations. Yet among developed nations such as Canada, less profound but still highly significant differences in health status indicators such as life expectancy, infant mortality, incidence of disease, and death from injuries exist.[38] An excellent example is comparison of health status differences and the hypothesized social determinants of these health status differences among Canada, the United States, and Sweden. [edit] Between developed countries. Scholarship has noted that the USA takes an especially laissez-faire approach to providing various forms of security (employment, food, income, and housing) and health and social services while Sweden’s welfare state makes extraordinary efforts to provide security and services.[39][40] The sources of these differences in public policy appear to be in differing commitments to citizen support informed by the political ideologies of governing parties within each nation.[41][42] Emerging scholarship is specifically focused on how national approaches to security provision to citizens influence health by shaping the quality of numerous social determinants of health. Nations such as Sweden whose policies reduce unemployment, minimize income and wealth inequality, and address numerous social determinants of health show evidence of improved population health using indicators such as infant mortality and life expectancy.[43] At the other end, nations with minimal commitments to such efforts such as the United States show rather worse indicators of population health.[44] [edit] Between developing and developed countries. Finally, poverty is an especially important indicator of how various social determinants of health combine to influence health. Using child – that is family – poverty rates as an important social determinants of both child and eventual health, Canada does not fare well in relation to European nations. People in rich countries live dramatically longer, healthier lives than people in poorer countries. Thus it can be argued, that it is the huge wealth inequalities between rich and poor countries, that is acting as a fundamental driver of poor global health. The causes of wealth inequalities are discussed elsewhere, and health advocacy groups are forming to lobby for recognition of these issues. To secure attention to the social determinants of health and build support for their strengthening, it is important to understand how social determinants of health come to influence health and cause disease. The very influential UK Black and The Health Divide reports considered two primary mechanisms for understanding this process: cultural/ behavioural and materialist/structuralist.[45] [edit] Cultural and Structuralist Approaches. The cultural/behavioural explanation was that individuals behavioural choices (e.g., tobacco and alcohol use, diet, physical activity, etc.) were responsible for their developing and dying from a variety of diseases. Both the Black and Health divide reports however, showed that behavioural choices are heavily structured by one’s material conditions of life. And—consistent with mounting evidence—these behavioural risk factors account for a relatively small proportion of variation in the incidence and death from various diseases. The materialist/structuralist explanation emphasizes the material conditions under which people live their lives. These conditions include availability of resources to access the amenities of life, working conditions, and quality of available food and housing among others. The author of the Health Divide concluded: The weight of evidence continues to point to explanations which suggest that socio-economic circumstances play the major part in subsequent health differences.[46] Despite this conclusion and increasing evidence in favour of this view, much of the Canadian public discourse on health and disease remains focused on life-style approaches to disease prevention.[47] These materialist/structuralist conceptualizations have been refined such that analysis is now focused upon three frameworks by which social determinants of health come to influence health.[48] These frameworks are: (a) materialist; (b) neo-materialist; and (c) psychosocial comparison. The materialist explanation is about how living conditions – and the social determinants of health that constitute these living conditions—shape health. The neo-materialist explanation extends the materialist analysis by asking how these living conditions come about. The psychosocial comparison explanation considers whether people compare themselves to others and how these comparisons affect health and wellbeing. In this argument individuals experience varying degrees of positive and negative exposures over their lives that accumulate to produce adult health outcomes.[49] Overall wealth of nations is a strong indicator of population health. But within nations, socio-economic position is a powerful predictor of health as it is an indicator of material advantage or disadvantage over the lifespan.[50] Material conditions of life determine health by influencing the quality of individual development, family life and interaction, and community environments. Material conditions of life lead to differing likelihood of physical (infections, malnutrition, chronic disease, and injuries), developmental (delayed or impaired cognitive, personality, and social development), educational (learning disabilities, poor learning, early school leaving), and social (socialization, preparation for work, and family life) problems.[44][49] Material conditions of life also lead to differences in psychosocial stress[51] The fight-or-flight reaction—chronically elicited in response to threats such as income, housing, and food insecurity, among others—weakens the immune system, leads to increased insulin resistance, greater incidence of lipid and clotting disorders, and other biomedical insults that are precursors to adult disease. Adoption of health-threatening behaviours is a response to material deprivation and stress.[52] Environments determine whether individuals take up tobacco, use alcohol, experience poor diets, and have low levels of physical activity. Tobacco and excessive alcohol use, and carbohydrate-dense diets are also means of coping with difficult circumstances.[53][54] Materialist arguments help us understand the sources of health inequalities among individuals and nations and the role played by the social determinants of health. [edit] Neo-materialist approach. Exposures to the material conditions of life are important for health, but why are these material conditions so unequally distributed among the Canadian population but less so elsewhere .[55][56] The neo-materialist approach is concerned with how nations, regions, and cities differ on how economic and other resources are distributed among the population.[57] Some jurisdictions have more equalitarian distribution of resources such that there are fewer poor people and the gaps that exist among the population in their exposures to the social determinants of health is narrower than places where there are more poor people and the gaps among the population are greater. In the USA, states and cities with more unequal distributions of income have more low-income people and greater income gaps between rich and poor. They invest less in public infrastructure such as education, health and social services, health insurance, supports for the unemployed and those with disabilities, and spend less on education and libraries. All of these issues contribute to the quality of the social determinants of health to which people are exposed. Such unequal jurisdictions have much poorer health profiles than more equalitarian places.[58][59] Canada has a smaller proportion of lower-income people, a smaller gap between rich and poor, and spends relatively more on public infrastructure than the U.S.[60] Not surprisingly, Canadians enjoy better health than Americans as measured by infant mortality rates, life expectancy, and death rates from childhood injuries.[10] Neither nation does as well as Sweden where distribution of resources is much more equalitarian, low-income rates are very low, and health indicators are among the best in the world. The neo-materialist view therefore, directs attention to both the effects of living conditions – the social determinants of health—on individuals health and the societal factors that determine the quality of the distribution of these social determinants of health. How a society decides to distribute resources among citizens is especially important. [edit] Social comparison approach. At the individual level, the perception and experience of one’s status in unequal societies lead to stress and poor health. Comparing their status, possessions, and other life circumstances to those better-off than themselves, individuals experience feelings of shame, worthlessness, and envy that have psychobiological effects upon health. These processes involve direct disease-producing effects upon neuro-endocrine, autonomic and metabolic, and immune systems.[51] These comparisons can also lead to attempts to alleviate such feelings by overspending, taking on additional employment that threaten health, and adopting health-threatening coping behaviours such as overeating and using alcohol and tobacco.[61] The argument here is that the social determinants of health play their role through citizens’ interpretations of their standings in the social hierarchy.[61][56] There are two mechanisms by which this occurs. At the communal level, widening and strengthening of hierarchy weakens social cohesion, a determinant of health.[62] Individuals become more distrusting and suspicious of others with direct stress-related effects on the body. Such attitudes can also weaken support for communal structures such as public education, health, and social programs. An exaggerated desire for tax reductions on the part of the public can weaken public infrastructure. This approach directs attention to the psychosocial effects of public policies that weaken the social determinants of health. But these effects may be secondary to how societies distribute material resources and provide security to its citizens – processes described in the materialist and neo-materialist approaches. Material aspects may be paramount and the stresses associated with deprivation simply add to the toll on individuals’ bodies. Traditional approaches to health and disease prevention have a distinctly non-historical here-and-now emphasis. Usually adults, and increasingly adolescents and youth are urged to adopt healthy lifestyles as a means of preventing the development of chronic diseases such as heart disease and diabetes, among others.[63][64] In contrast to these approaches, life-course approaches emphasize the accumulated effects of experience across the life span in understanding the maintenance of health and the onset of disease. It has been argued: [edit] Life-course perspective. The prevailing aetiological model for adult disease which emphasizes adult risk factors, particularly aspects of adult life style, has been challenged in recent years by research that has shown that poor growth and development and adverse early environmental conditions are associated with an increased risk of adult chronic disease Kuh, D., & Ben-Shilmo, Y. (Eds.). (1997). A life course approach to chronic disease epidemiology. Oxford, UK: Oxford University Press,p.3. More specifically, it is apparent that the economic and social conditions—the social determinants of health—under which individuals live their lives have a cumulative effect upon the probability of developing any number of diseases. This has been repeatedly demonstrated in longitudinal studies—the U.S. National Longitudinal Survey, the West of Scotland Collaborative Study, Norwegian and Finnish linked data—which follow individuals across their lives.[65] This has been most clearly demonstrated in the case of heart disease and stroke.[25] And most recently, studies into the childhood and adulthood antecedents of adult-onset diabetes show how adverse economic and social conditions across the life span predispose individuals to this disorder.[28][66][40] A recent volume brings together some of the important work concerning the importance of a life-course perspective for understanding the importance of social determinants.[67] Adopting a life-course perspective directs attention to how social determinants of health operate at every level of development—early childhood, childhood, adolescence, and adulthood—to both immediately influence health as well as provide the basis for health or illness during later stages of the life course. Hertzman outlines three health effects that have relevance for a life-course perspective.[68] Latent effects are biological or developmental early life experiences that influence health later in life. Low birth weight, for instance, is a reliable predictor of incidence of cardiovascular disease and adult-onset diabetes in later life. Experience of nutritional deprivation during childhood has lasting health effects. Pathway effects are experiences that set individuals onto trajectories that influence health, well-being, and competence over the life course. As one example, children who enter school with delayed vocabulary are set upon a path that leads to lower educational expectations, poor employment prospects, and greater likelihood of illness and disease across the lifespan. Deprivation associated with poor-quality neighbourhoods, schools, and housing sets children off on paths that are not conducive to health and well-being. Cumulative effects are the accumulation of advantage or disadvantage over time that manifests itself in poor health. These involve the combination of latent and pathways effects. Adopting a life-course perspective directs attention to how social determinants of health operate at every level of development—early childhood, childhood, adolescence, and adulthood—to both immediately influence health and provide the basis for health or illness later in life. Much social determinants of health research simply focuses on determining the relationship between a social determinant of health and health status. So a researcher may document that lower income is associated with adverse health outcomes among parents and their children. Or a researcher may demonstrate that food insecurity is related to poor health status among parents and children as is living in crowded housing, and so on. This is what is termed a depoliticized approach in that it says little about how these poor-quality social determinants of health come about.[69] [edit] Public policy. Social determinants of health do not exist in a vacuum. Their quality and availability to the population are usually a result of public policy decisions made by governing authorities. As one example, consider the social determinant of health of early life. Early life is shaped by availability of sufficient material resources that assure adequate educational opportunities, food and housing among others. Much of this has to do with the employment security and the quality of working conditions and wages. The availability of quality, regulated childcare is an especially important policy option in support of early life. [70] These are not issues that usually come under individual control. A policy-oriented approach places such findings within a broader policy context. Yet it is not uncommon to see governmental and other authorities individualize these issues. Governments may choose to understand early life as being primarily about parental behaviours towards their children. They then focus upon promoting better parenting, assist in having parents read to their children, or urge schools to foster exercise among children rather than raising the amount of financial or housing resources available to families. Indeed, for every social determinant of health, an individualized manifestation of each is available. There is little evidence to suggest the efficacy of such approaches in improving the health status of those most vulnerable to illness in the absence of efforts to modify their adverse living conditions.[71] One way to think about this is to consider the idea of the welfare state and the political ideologies that shape its form in Canada and elsewhere. The concept of the welfare state is about the extent to which governments – or the state – use their power to provide citizens with the means to live secure and satisfying lives. Every developed nation has some form of the welfare state. [edit] Politics and political ideology. Two literature s inform this analysis. The first concerns the three forms of the modern welfare state. Esping-Andersen identifies three distinct clusters of welfare regimes among wealthy developed nations: Social Democratic (e.g., Sweden, Norway, Denmark, and Finland), Liberal (USA, UK, Canada, Ireland), and Conservative (France, Germany, Netherlands, and Belgium, among others).[72][73] There is high government intervention and strong welfare systems in the social democratic countries and rather less in the liberal. Conservative nations fall midway between these others in service provision and citizen supports. Social democratic nations have very well developed welfare states that provide a wide range of universal and generous benefits. They expend more of national wealth to supports and services. They are proactive in developing labour, family-friendly, and gender equity supporting policies. Liberal nations spend rather less on supports and services. They offer modest universal transfers and modest social-insurance plans. Benefits are provided primarily through means-tested assistance whereby these benefits are only provided to the least well-off. Navarro and colleagues provide empirical support for the hypotheses that the social determinants of health and health status outcomes are of higher quality in the social democratic rather than the liberal nations.[74][42] Some of these indicators are spending on supports and services, equitable distribution of income, and wealth and availability of services in support of families and individuals. Health indicators include life expectancy and infant mortality. A particularly important issue that is emerging is whether any particular analysis of social determinants of health is de-politicized or not. A de-politicized approach is one that fails to take account of the fact that the quality of the social determinants of health to which citizens in a jurisdiction are exposed to is shaped by public policy created by governments. And governments of course are controlled by political parties who come to power with a set of ideological beliefs concerning the nature of society and the role of governments. Could this general approach to welfare provision shape Canadian receptivity to the concepts developed in this volume And if so, what can be done to improve receptivity to and implementation of these concepts The final chapter of this volume revisits these issues. Such analyses that recognize the role played by politics outline the particular importance of having social democratic political parties in power. Nations that have had longer periods of social democratic influence such as Norway, Finland, Sweden, and Denmark have government policymaking that is remarkably consistent with social determinants of health concepts. Nations such as the USA and Canada,dominated by liberal and neo-liberal governing parties, much less so. The weight of the evidence suggests that the SDOH have a direct impact on the health of individuals and populations, are the best predictors of individual and population health, structure lifestyle choices, and interact with each other to produce health (Raphael, 2003). In terms of the health of populations, it is well known that disparities-the size of the gap or inequality in social and economic status between groups within a given population-greatly affect the health status of the whole. The larger the gap, the lower the health status of the overall population.[53][54] An example of SDOH, applicable to the United States, is shown in the graph. It shows self-reported health as it relates to income level and political party identification (Democrat vs. Republican).[77] A wealth of evidence from Canada and other countries supports the notion that the socioeconomic circumstances of individuals and groups are equally or more important to health status than medical care and personal health behaviours, such as smoking and eating patterns. [75][76] Health literacy. Health equity. [edit] See also. Global health. Population health. Diseases of poverty. Diseases of affluence. Whitehall Study. Hopkins Center for Health Disparities Solutions. Population Health Forum. Center for Minority Health. Social epidemiology. Social determinants of obesity. Race and health. Medical sociology. Medical anthropology. Unnatural Causes: Is Inequality Making Us Sick Michael Marmot. [edit] References. Dennis Raphael. Richard G. Wilkinson. ^ McKeown, T., & Record, R. G. (1975). An interpretation of the decline in mortality in England and Wales during the twentieth century. Population Studies, 29, ^ McKeown, T. (1976). The Role of Medicine: Dream, Mirage, or Nemesis. London UK: Neufeld Provincial Hospitals Trust. ^ a b McKinlay, J., & McKinlay, S. M. (1987). Medical measures and the decline of mortality. In H. D. Schwartz (Ed.), Dominant issues in medical sociology (2nd edition ed.). New York: Random House. ^ Canadian Population Health Initiative. (2004). Improving the Health of Canadians. Ottawa: CPHI. ^ a b c d Wilkins, R., Berthelot, J.-M., & Ng, E. (2002). Trends in mortality by neighbourhood income in urban Canada from 1971 to Health Reports (Stats Can), 13(Supplement), ^ Health Canada. (1999). Toward a Healthy Future: Second Report on the Health of Canadians. Retrieved August, 2002, from ^ Canadian Population Health Initiative. (2008). Reducing Gaps in Health: A Focus on Socio-Economic Status in Urban Canada. Ottawa: Canadian Population Health Initiative. ^ a b Siddiqi, A., & Hertzman, C. (2007). Towards an epidemiological understanding of the effects of long-term institutional changes on population health: A case study of Canada versus the USA. Social Science & Medicine, 64(3), ^ Raphael, D. (2007). Interactions with the health and service sector. In D. Raphael (Ed.), Poverty and policy in Canada: Implications for health and quality of life. (pp ). Toronto: Canadian Scholars Press. ^ McGibbon, E. (2008). Health and health care: A human rights perspective. In D. Raphael (Ed.), Social Determinants of Health: Canadian Perspectives (2nd ed., pp ). Toronto: Canadian Scholars Press. ^ Marmot, M., Shipley, M., Brunner, E., & Hemingway, H. (2001). Relative Contribution of Early Life and Adult Socioeconomic Factors to Adult Morbidity in the Whitehall II Study. Journal of Epidemiology and Community Health, 2001(55), 5. ^ a b Raphael, D., Macdonald, J., Labonte, R., Colman, R., Hayward, K., & Torgerson, R. (2004). Researching income and income distribution as a determinant of health in Canada: Gaps between theoretical knowledge, research practice, and policy implementation. Health Policy, 72, ^ Raphael, D. (2007). Poverty and Health: Mechanisms and Pathways. In D. Raphael (Ed.), Poverty and Policy in Canada: Implications for Health and Quality of Life (pp ). Toronto: Canadian Scholars Press. ^ Nettleton, S. (1997). Surveillance, health promotion and the formation of a risk identity. In M. Sidell, L. Jones, J. Katz & A. Peberdy (Eds.), Debates and Dilemmas in Promoting Health (pp ). London, UK: Open University Press. ^ a b Benzeval, M., Dilnot, A., Judge, K., & Taylor, J. (2001). Income and health over the lifecourse: Evidence and policy implications. In H. Graham (Ed.), Understanding Health Inequalities (pp ). Buckingham, UK: Open University Press. ^ Raphael, D., Labonte, R., Colman, R., Torgeson, R., Hayward, K., & Macdonald, J. (2006). Income and health research in Canada: Needs, gaps, and opportunities. Canadian Journal of Public Health, 97(Supplement #3), s16-s23. ^ Raphael, D. (2007). Who is poor in Canada In D. Raphael (Ed.), Poverty and policy in Canada: Implications for health and quality of life, (pp ). Toronto: Canadian Scholars Press. ^ Benzeval, M., & Judge, K. (2001). Income and health: The time dimension. Social Science & Medicine, 52, ^ Shields, M., & Tremblay, S. (2002). The Health of Canada s Communities. Health Reports. Supplement, 13(July), ^ Judge, K., & Paterson, I. (2002). Treasury Working Paper: Poverty, Income Inequality and Health. Wellington, NZ: Government of New Zealand. ^ a b Davey Smith, G., & Hart, C. (2002). Life-Course Approaches to Socio-Economic and Behavioural Influences on Cardiovascular Disease Mortality. American Journal of Public Health, 92(8), ^ Raphael, D., Anstice, S., & Raine, K. (2003). The social determinants of the incidence and management of Type 2 Diabetes Mellitus: Are we prepared to rethink our questions and redirect our research activities Leadership in Health Services, 16, ^ Roux, A., Merkin, S., & Arnett, D. (2001). Neighbourhood of Residence and Incidence of Coronary Heart Disease. New England Journal of Medicine, 345, ^ Lantz, P. M., House, J. S., Lepkowski, J. M., Williams, D. R., Mero, R. P., & Chen, J. J. (1998). Socioeconomic factors, health behaviors, and mortality. Journal of the American Medical Association, 279(21), ^ a b Raphael, D., & Farrell, E. S. (2002). Beyond medicine and lifestyle: Addressing the societal determinants of cardiovascular disease in North America. Leadership in Health Services, 15, 1-5. ^ a b Lawlor, D., Ebrahim, S., & Smith, G. D. (2002). Socioeconomic position in childhood and adulthood and insulin resistance: cross sectional survey using data from British women s heart and health study. British Medical Journal, 325(12), ^ Davey Smith, G., Ben-Shlomo, Y., & Lynch, J. (2002). Life course approaches to inequalities in coronary heart disease risk. In S. A. Stansfeld & M. Marmot (Eds.), Stress and the Heart: Psychosocial Pathways to Coronary Heart Disease (pp ). London, UK: BMJ Books. ^ Chaufan, C. (2008). What does justice have to do with it A bioethical and sociological perspective on the diabetes epidemic. Bioethical Issues, Sociological Perspectives, 9, ^ Eriksson, J., Forsen, T., Tuomilehto, J., Winter, P., Osmond, C., & Barker, D. (1999). Catch-up growth in childhood and death from coronary heart disease: longitudinal study. BMJ - Clinical Research, 318(7181), ^ Barker, D. J., Osmond, C., & Simmonds, M. (1989). Weight in infancy and death from ischemic heart disease. The Lancet, 2, ^ Benzeval, M., Judge, K., & Whitehead, M. (1995). Tackling Inequalities in Health: An Agenda for Action. London: Kings Fund. ^ Eriksson, J. G., Forsen, T., Tuomilehto, J., Osmond, C., & Barker, B. J. (2001). Early Growth and Coronary Heart Disease in later life: Longitudinal Study. British Medical Journal, 322, ^ Ross, D. P., Roberts, P., & Scott, K. (2000). Family income and child well-being. ISUMA, 1(2), ^ Ross, D. P., & Roberts, P. (1999). Income and Child Well-Being: A New Perspective on the Poverty Debate. Ottawa, Canada: Canadian Council on Social Development. ^ Canadian Institute on Children s Health. (2000). The Health of Canada s Children: A CICH Profile 3rd Edition. Ottawa, Canada: Canadian Institute on Children s Health. ^ Organisation for Economic Cooperation and Development. (2007). Health at a Glance 2007, OECD Indicators. Paris: Organisation for Economic Cooperation and Development. ^ L. Donaldson, Ten Tips for Better Health (London: Stationary Office, 1999). ^ Willms, J. D. (Ed.). (2002). Vulnerable Children: Findings from Canada s National Longitudinal Survey. Edmonton, AB: University of Alberta Press. ^ Burstrom, B., Diderichsen, F., Ostlin, P., & Ostergren, P. O. (2002). Sweden. In J. Mackenbach & M. Bakker (Eds.), Reducing Inequalities in Health: A European Perspective (pp ). London UK: Routledge. ^ a b Navarro, V., & Shi, L. (2002). The political context of social inequalities and health. In V. Navarro (Ed.), The Political Economy of Social Inequalities: Consequences for Health and Quality of Life (pp ). Amityville, NY: Baywood. ^ Bambra, C. (2004). The worlds of welfare: illusory and gender blind Social Policy and Society, 3(3), ^ a b Raphael, D., & Bryant, T. (2006). The State s role in promoting population health: Public health concerns in Canada, USA, UK, and Sweden. Health Policy, 78, ^ Townsend, P., Davidson, N., & Whitehead, M. (Eds.). (1992). Inequalities in Health: the Black Report and the Health Divide. New York: Penguin. ^ a b Raphael, D. (2007c). Poverty and Health. In D. Raphael (Ed.), Poverty and Policy in Canada: Implications for Health and Quality of Life (pp ). Toronto: Canadian Scholars Press. ^ Diderichsen, F., Whitehead, M., Burstrom, B., & Aberg, M. (2001). Sweden and Britain: The impact of policy context on inequities in health. In T. Evans, M. Whitehead, F. Diderichsen, A. Bhuya & M. Wirth (Eds.), Challenging Inequities in Health: from Ethics to Action (pp ). New York: Oxford University Press. ^ Whitehead, M. (1992). The health divide. In P. Townsend, N. Davidson & M. Whitehead (Eds.), Inequalities in Health: the Black Report and the Health Divide (pp ). New York: Penguin. ^ a b Shaw, M., Dorling, D., Gordon, D., & Smith, G. D. (1999). The Widening Gap: Health Inequalities and Policy in Britain. Bristol, UK: The Policy Press. ^ Bartley, M. (2003). Understanding Health Inequalities. Oxford UK: Polity Press. ^ Raphael, D. (2008a). Grasping at straws: A recent history of health promotion in Canada. Critical Public Health, 18(4), ^ Jarvis, M. J., & Wardle, J. (2003). Social patterning of individual health behaviours: the case of cigarette smoking. In M. G. ^ a b Brunner, E., & Marmot, M. G. (2006). Social organization, stress, and health. In M. G. Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp. 6-30). Oxford: Oxford University Press. ^ Graham, H. (2007). Unequal Lives: Health and Socioeconomic Inequalities. New York: Open University Press. ^ a b Wilkinson, R. G. (1996). Unhealthy Societies: The Afflictions of Inequality. New York: Routledge. ^ a b Tarlov, A. (1996). Social determinants of health: The sociobiological translation. In D. Blane, E. Brunner & R. Wilkinson (Eds.), Health and Social Organization: Towards a Health Policy for the 21st Century (pp ). London UK: Routledge. ^ Graham, H. (2004). Social determinants and their unequal distribution: Clarifying policy understandings. Milbank Quarterly, 82(1), ^ a b Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp ). Oxford, UK: Oxford University Press. ^ Lynch, J. W., Kaplan, G. A., Pamuk, E. R., Cohen, R., Heck, C., Balfour, J., et al. (1998). Income inequality and mortality in metropolitan areas of the United States. American Journal of Public Health, 88, ^ Kaplan, G. A., Pamuk, E. R., Lynch, J. W., Cohen, J. W., & Balfour, J. L. (1996). Income Inequality and Mortality in The United States. BMJ, 312, ^ Lynch, J. W., Smith, G. D., Kaplan, G. A., & House, J. S. (2000). Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ, 320, ^ Ross, N., Wolfson, M., Dunn, J., Berthelot, J. M., Kaplan, G., & Lynch, J. (2000). Relation between income inequality and mortality in Canada and in the United States: Cross sectional assessment using census data and vital statistics. BMJ, 320(7239), ^ Chronic Disease Prevention Alliance of Canada. (2003). Who We Are. Retrieved April 16, 2003, from ^ Kawachi, I., & Kennedy, B. P. (1997). Socioeconomic determinants of health : Health and social cohesion: why care about income inequality BMJ, 314(7086), ^ a b Kawachi, I., & Kennedy, B. (2002). The Health of Nations: Why Inequality Is Harmful to Your Health. New York: New Press. ^ Raphael, D., Anstice, S., & Raine, K. (2003). The social determinants of the incidence and management of Type 2 Diabetes Mellitus: Are we prepared to rethink our questions and redirect our research activities Leadership in Health Services, 16, ^ Blane, D. (2006). The life course, the social gradiant and health. In M. G. Marmot & R. G. Wilkinson (Eds.), Social Determinants of Health (2nd ed., pp ). Oxford: Oxford University Press. ^ Health Canada. (2003). Healthy Living Strategy. Retrieved April 16, 2003, from ^ Davey Smith, G. (Ed.). (2003). Inequalities in Health: Life Course Perspectives. Bristol UK: Policy Press. ^ Esping-Andersen, G. (2002). A child-centred social investment strategy. In G. Esping-Andersen (Ed.), Why we need a new welfare state (pp ). Oxford UK: Oxford University Press. ^ Raphael, D., & Bryant, T. (2002). The limitations of population health as a model for a new public health. Health Promotion International, 17, ^ Hertzman, C. (2000). The case for an early childhood development strategy. Isuma, Autumn. ^ Esping-Andersen, G. (1999). Social Foundations of Post-Industrial Economies. New York: Oxford University Press. ^ Esping-Andersen, G. (1990). The Three Worlds of Welfare Capitalism. Princeton: Princeton University Press. ^ Raphael, D. (2001). Inequality is Bad for our Hearts: Why Low Income and Social Exclusion are Major Causes of Heart Disease in Canada, from ^ Navarro, V. (Ed.). (2004). The Political and Social Contexts of Health. Amityville NY: Baywood Press. ^ Fried, Joseph, Democrats and Republicans - Rhetoric and Reality (New York: Algora Publishing, 2008), 25. ^ Restrepo, H. E. (2000). Health Promotion: An Anthology. In H. E. Restrepo (Ed.), (pp. ix-xi). Washington, DC: Pan American Health Organization. ^ Evans, R. G., Barer, M. L., & Marmor, T. R. (1994). Why Are Some People Healthy and Others Not : The Determinants of Health of Populations. New York: Aldine de Gruyter. Health Canada. (2001). The Population Health Template: Key Elements and Actions That Define A Population Health Approach. Retrieved June, 2002, from Raphael, D. (2010). About Canada: Health and Illness, Retrieved August, 2010, from [edit] Further reading. Raphael, D. (2008c). Public policy and population health in the USA: Why is the public health community missing in action International Journal of Health Services, 38, Social Determinants of Health: The Canadian Facts. [edit] External links. Social Determinants of Health: Canadian Perspectives provides the latest developments and is available at Excerpts are available at About Canada: Health and Illness. Population Health Forum website. World Health Organization: Commission on Social Determinants of Health. Public Health Agency of Canada: What determines health - Key Determinants. CBC Ideas - Sick People or Sick Societies Part 1 and Part 2. VIDEO: Health Status Disparities in the US featuring Paula Braveman, Gregg Bloche, George Kaplan, Thomas Ricketts, Mary Lou deLeon Siantz, and David Williams.")
16
Determinanty zdraví a nemoci
Životní prostředí (ovzduší,voda, záření, chemické látky, biologické faktory-infekce) Životní styl (kouření, způsob stravování, pohybové aktivity, sociální a ekonomické faktory-příjem, vzdělání, typ práce) Genetické vlohy (vrozené nebo v průběhu života vzniklé vady nebo dispozice ke vzniku nemoci) Zdravotnické služby (ambulantní služby, nemocniční služby, lékárny, lékařská služba první pomoci) Váha vlivu těchto čtyř determinant zdraví je v různých společnosti odlišná
 Životní styl (kouření, způsob stravování, pohybové aktivity, sociální a ekonomické faktory-příjem, vzdělání, typ práce) Genetické vlohy (vrozené nebo v průběhu života vzniklé vady nebo dispozice ke vzniku nemoci) Zdravotnické služby (ambulantní služby, nemocniční služby, lékárny, lékařská služba první pomoci) Váha vlivu těchto čtyř determinant zdraví je v různých společnosti odlišná.")
17
Determinanty zdraví a nemoci
Váha vlivu determinant zdraví, příklad pro vyspělý stát: 50% Životní styl 20% Genetické vlohy 15% Zdravotnické služby 15% Životní prostředí Poznámka: V jiných státech a za jiných společenských podmínek jsou váhy vlivu determinant odlišné

18
Model determinant zdraví a nemoci Zdroj: Detels, R. (2004) a spol
Model determinant zdraví a nemoci Zdroj: Detels, R. (2004) a spol. Oxford Textbook of Public Health. Oxford University Press, Oxford, 4th edition, str. 84
 a spol. Oxford Textbook of Public Health. Oxford University Press, Oxford, 4th edition, str. 84.")
19
Influenční model determinant zdraví a nemoci
Sociální faktory Psychologické dispozice Fyzikální a chemické faktory Ekonomické faktory Biologické dispozice Interakce jedince s prostředím Napodobování Životní styl Učení se Podpora zdraví Cyklus podpory zdraví Zdraví Vyhledání péče Cyklus zdravotnické péče Nemoc Zdravotnická péče Výsledek péče Kvalita života Prosperita a blahobyt [Zdroj: Noack, 1997], NOACK, R.H. 4th. International Conference on Health Promotion. Jakarta, Indonesia, 21 – 25 July 1997

20
„Cibulovitý“ model determinant zdraví
Zdroj: Drbal

21
Determinanty zdraví a nemoci Otázky
Co vyplývá z předchozího zjištění váhy vlivu jednotlivých determinant zdraví pro tvorbu zdravotní politiky? Jaké jsou naše možnosti (metody) poznání vlivu determinant zdraví a nemoci?
 poznání vlivu determinant zdraví a nemoci")
22
Determinanty zdraví a investice do zdraví
Produkce zdraví je ovlivněna více faktory. Ne jenom zdravotnickými službami!!!!! Source: The contribution of health to the economy in the European Union. European Communities, 2005

23
Source: D.Cutler, Production of Health, Manuscript 2002, data USA

26
Social determinants of health (agenda WHO)
The social determinants of health are the conditions in which people are born, grow, live, work and age, including the health system. These circumstances are shaped by the distribution of money, power and resources at global, national and local levels, which are themselves influenced by policy choices. The social determinants of health are mostly responsible for health inequities - the unfair and avoidable differences in health status seen within and between countries. Responding to increasing concern about these persisting and widening inequities, WHO established the Commission on Social Determinants of Health (CSDH) in 2005 to provide advice on how to reduce them. The Commission's final report was launched in August 2008, and contained three overarching recommendations: 1. Improve daily living conditions 2. Tackle the inequitable distribution of power, money, and resources 3. Measure and understand the problem and assess the impact of action
 in 2005 to provide advice on how to reduce them. The Commission s final report was launched in August 2008, and contained three overarching recommendations: 1. Improve daily living conditions 2. Tackle the inequitable distribution of power, money, and resources 3. Measure and understand the problem and assess the impact of action.")
27
Social determinants of health Publications
Key documents :: Closing the gap in a generation: Health equity through action on the social determinants of health The Commission's final report contains recommendations for action, based on the evidence gathered across all the Commission’s work streams. :: Interim Statement of the Commission on Social Determinants of Health 2007 The Interim Statement sets out the Commission’s vision and goals, the problems it seeks to ameliorate, and the intellectual foundation for a social determinants approach. Most downloaded :: 1 Closing the gap in a generation: Health equity through action on the social determinants of health Final report of the Commission :: 2 Developing an evidence base for political action [pdf 618kb] Final report of the Measurement and Evidence Knowledge Network :: 3 Social determinants of health inequalities [pdf 86kb] Michael Marmot - article from The Lancet :: 4 Employment conditions and health inequalities [pdf 1.30Mb] Final report of the Employment Conditions Knowledge Network

28
Péče o zdraví PÉČE O ZDRAVÍ (zdravotní péče) činnost společnosti, spočívající v soustavě politických, ekonomických, kulturně výchovných a zdravotnických opatření, jejichž cílem je rozvíjet, upevňovat, chránit a navracet lidem zdraví a pracovní schopnost, prodlužovat lidský život, činit jej aktivní, spokojený a šťastný, a zabezpečovat zdravý vývoj nových generací.
 činnost společnosti, spočívající v soustavě politických, ekonomických, kulturně výchovných a zdravotnických opatření, jejichž cílem je rozvíjet, upevňovat, chránit a navracet lidem zdraví a pracovní schopnost, prodlužovat lidský život, činit jej aktivní, spokojený a šťastný, a zabezpečovat zdravý vývoj nových generací.")
29
Zdravotnictví ZDRAVOTNICTVÍ je soustava odborných zařízení, lidských zdrojů, poskytovatelů služeb a dalších subjektů a jim odpovídajících činností, jež společnost vytváří na základě výsledků lékařských a jiných věd, jako specifický nástroj poznání a uspokojování zdravotních potřeb obyvatelstva.

30
Definice nemoci* NEMOC ve fyzikálním smyslu bývá nejčastěji chápána jako projev mikroskopické nebo hrubé poruchy struktury buněk a tkání, doprovázený změnami biochemického složení a fyziologických funkcí jednotlivých orgánů nebo celého tělesného systému, které přesáhly hranici adaptability. Nemoc neboli choroba či onemocnění je patologický stav těla nebo mysli, který je projevem změny funkcí buněk a v důsledku i morfologickým poškozením těchto buněk, tkání a orgánů. Podle normativní definice zdraví a nemoci je nemocí pouze takový stav, který nemocnému jedinci způsobuje subjektivní potíže, tato definice ale z lékařského hlediska nepokrývá všechny nemoci - příkladem je vysoký krevní tlak nebo některá nádorová onemocnění. Tato definice je tedy vhodná jen pro rozvinutá stadia nemoci. Funkcionalistická definice zdraví a nemoci definuje některé funkce organismu jako správné a jiné už jako patologické, bez ohledu na to, jestli ty patologické způsobují nějaké subjektivní potíže. Problémem tohoto přístupu je ale stanovení „normálnosti“ funkcí, protože u většiny nemocí je přesun od fyziologických hodnot k patologickým plynulý. Termín onemocnění je někdy používáno jako synonymum nemoci, jindy pro označení počátku nemoci nebo pro zdůraznění toho, že stav není konstituční, trvalou vlastností organismu.[zdroj?] Infekční neboli nakažlivá nemoc je infekční onemocnění, jehož původce je schopný přenosu z organismu na organismus (např. chřipka, mor). DISEASE From Wikipedia, the free encyclopedia It has been suggested that Illness be merged into this article or section. (Discuss) Proposed since May "Medical condition" redirects here. For medical condition terminology, see Medical state. For other uses, see Disease (disambiguation). A disease is an abnormal condition affecting the body of an organism. It is often construed to be a medical condition associated with specific symptoms and signs.1 It may be caused by external factors, such as infectious disease, or it may be caused by internal dysfunctions, such as autoimmune diseases. In humans, "disease" is often used more broadly to refer to any condition that causes pain, dysfunction, distress, social problems, or death to the person afflicted, or similar problems for those in contact with the person. In this broader sense, it sometimes includes injuries, disabilities, disorders, syndromes, infections, isolated symptoms, deviant behaviors, and atypical variations of structure and function, while in other contexts and for other purposes these may be considered distinguishable categories. Diseases usually affect people not only physically, but also emotionally, as contracting and living with many diseases can alter one's perspective on life, and their personality. Death due to disease is called death by natural causes. There are four main types of disease: pathogenic disease, deficiency disease, hereditary disease, and physiological disease. Diseases can also be classified as communicable and non-communicable disease. In many cases, the terms disease, disorder, morbidity and illness are used interchangeably.2 In some situations, specific terms are considered preferable. The term disease broadly refers to any condition that impairs normal function. Commonly, this term is used to refer specifically to infectious diseases, which are clinically evident diseases that result from the presence of pathogenic microbial agents, including viruses, bacteria, fungi, protozoa, multicellular organisms, and aberrant proteins known as prions. An infection that does not and will not produce clinically evident impairment of normal functioning, such as the presence of the normal bacteria and yeasts in the gut, is not considered a disease; by contrast, an infection that is asymptomatic during its incubation period, but expected to produce symptoms later, is usually considered a disease. Non-infectious diseases are all other diseases, including most forms of cancer, heart disease, and genetic disease. Illness and sickness are generally used as synonyms for disease.3 However, this term is occasionally used to refer specifically to the patient's personal experience of their disease.45 In this model, it is possible for a person to be diseased without being ill (to have an objectively definable, but asymptomatic, medical condition), and to be ill without being diseased (such as when a person perceives a normal experience as a medical condition, or medicalizes a non-disease situation in his or her life). Illness is often not due to infection but a collection of evolved responses, sickness behavior, by the body which aids the clearing of infection. Such aspects of illness can include lethargy, depression, anorexia, sleepiness, hyperalgesia, and inability to concentrate.678 In medicine, a disorder is a functional abnormality or disturbance. Medical disorders can be categorized into mental disorders, physical disorders, genetic disorders, emotional and behavioral disorders, and functional disorders. The term disorder is often considered more value-neutral and less stigmatizing than the terms disease or illness, and therefore is preferred terminology in some circumstances. In mental health, the term mental disorder is used as a way of acknowledging the complex interaction of biological, social, and psychological factors in psychiatric conditions. However, the term disorder is also used in many other areas of medicine, primarily to identify physical disorders that are not caused by infectious organisms, such as metabolic disorders. A medical condition is a broad term that includes all diseases and disorders. While the term medical condition generally includes mental illnesses, in some contexts the term is used specifically to denote any illness, injury, or disease except for mental illnesses. The Diagnostic and Statistical Manual of Mental Disorders (DSM), the widely used psychiatric manual that defines all mental disorders, uses the term general medical condition to refer to all diseases, illnesses, and injuries except for mental disorders.9 This usage is also commonly seen in the psychiatric literature. Some health insurance policies also define a medical condition as any illness, injury, or disease except for psychiatric illnesses.10 As it is more value-neutral than terms like disease, the term medical condition is sometimes preferred by people with health issues that they do not consider to be deleterious. On the other hand, by emphasizing the medical nature of the condition, this term is sometimes rejected, such as by proponents of the autism rights movement. The term medical condition is used as a synonym for medical state, where it describes a patient's current state, as seen from a medical standpoint. This usage is seen in statements that describe a patient as being "in critical condition", for example. Morbidity (from Latin morbidus, meaning "sick, unhealthy") is a diseased state, disability, or poor health due to any cause.11 The term may be used to refer to the existence of any form of disease, or to the degree that the health condition affects the patient. Among severely ill patients, the level of morbidity is often measured by ICU scoring systems. Comorbidity is the simultaneous presence of two or more medical conditions, such as schizophrenia and substance abuse. In epidemiology and actuarial science, the term morbidity rate can refer to either the incidence rate, or the prevalence of a disease or medical condition. This measure of sickness is contrasted with the mortality rate of a condition, which is the proportion of people dying during a given time interval. Syndrome (from Ancient Greek syn, meaning "together", and dramein, meaning "run") is a set of symptoms occurring together. Predisease is a type of or medicalization in which currently healthy people with risk factors for disease, but no evidence of actual disease, are told that they are sick. Prediabetes and prehypertension are common examples. Labeling a healthy person with predisease can result in overtreatment, such as taking drugs that only help people with severe disease, or in useful preventive measures, such as motivating the person to get a healthful amount of physical exercise.12 "Flareup" redirects here. For the Transformers character, see Flareup (Transformers). In an infectious disease, the incubation period is the time between infection and the appearance of symptoms. The latency period is the time between infection and the ability of the disease to spread to another person, which may precede, follow, or be simultaneous with the appearance of symptoms. Some viruses also exhibit a dormant phase, called viral latency, in which the virus hides in the body in an inactive state. For example, varicella zoster virus causes chickenpox in the acute phase; after recovery from chickenpox, the virus may remain dormant in nerve cells for many years, and later cause herpes zoster (shingles). A cure is the end of a medical condition or a treatment that is very likely to end it, while remission refers to the disappearance, possibly temporarily, of symptoms. Complete remission is the best possible outcome for incurable diseases. A flare-up can refer to either the recurrence of symptoms or an onset of more severe symptoms. A refractory disease is a disease that resists treatment, especially an individual case that resists treatment more than is normal for the specific disease in question. Progressive disease is a disease whose typical natural course is the worsening of the disease until death, serious debility, or organ failure occurs. Slowly progressive diseases are also chronic diseases; many are also degenerative diseases. The opposite of progressive disease is stable disease or static disease: a medical condition that exists, but does not get better or worse. A localized disease is one that affects only one part of the body, such as athlete's foot or an eye infection. A disseminated disease has spread to other parts; with cancer, this is usually called metastatic disease. A systemic disease is a disease that affects the entire body, such as influenza or high blood pressure. Main article: Transmission (medicine) Only some diseases such as influenza are contagious and commonly believed to be infectious. The micro-organisms that cause these diseases are known as pathogens and include varieties of bacteria, viruses, protozoa and fungi. Infectious diseases can be transmitted, e.g. by hand-to-mouth contact with infectious material on surfaces, by bites of insects or other carriers of the disease, and from contaminated water or food (often via faecal contamination), etc. In addition, there are sexually transmitted diseases. In some cases, micro-organisms that are not readily spread from person to person play a role, while other diseases can be prevented or ameliorated with appropriate nutrition or other lifestyle changes. Some diseases, such as most (but not all) forms of cancer, heart disease and mental disorders, are non-infectious diseases. Many non-infectious diseases have a partly or completely genetic basis (see genetic disorder) and may thus be transmitted from one generation to another. Social determinants of health are the social conditions in which people live which determine their health. Illnesses are generally related to social, economic, political, and environmental circumstances. Social determinants of health have been recognized by several health organizations such as the Public Health Agency of Canada and the World Health Organization to greatly influence collective and personal well-being. The World Health Organization's Social Determinants Council also recognizes Social determinants of health in poverty. When the cause of a disease is poorly understood, societies tend to mythologize the disease or use it as a metaphor or symbol of whatever that culture considers to be evil. For example, until the bacterial cause of tuberculosis was discovered in 1882, experts variously ascribed the disease to heredity, a sedentary lifestyle, depressed mood, and overindulgence in sex, rich food, or alcohol—all the social ills of the time.13 Disease burden is the impact of a health problem in an area measured by financial cost, mortality, morbidity, or other indicators. There are several measures used to quantify the burden imposed by diseases on people. The years of potential life lost (YPLL) is a simple estimate of the number of years that a person's life was shortened due to a disease. For example, if a person dies at the age of 65 from a disease, and would probably have lived until age 80 without that disease, then that disease has caused a loss of 15 years of potential life. YPLL measurements do not account for how disabled a person is before dying, so the measurement treats a person who dies suddenly and a person who died at the same age after decades of illness as equivalent. In 2004, the World Health Organization calculated that 932 million years of potential life were lost to premature death.14 The quality-adjusted life year (QALY) and disability-adjusted life year (DALY) metrics are similar, but take into account whether the person was healthy after diagnosis. In addition to the number of years lost due to premature death, these measurements add part of the years lost to being sick. Unlike YPLL, these measurements show the burden imposed on people who are very sick, but who live a normal lifespan. A disease that has high morbidity, but low mortality, will have a high DALY and a low YPLL. In 2004, the World Health Organization calculated that 1.5 billion disability-adjusted life years were lost to disease and injury.14 Disease categoryPercent of all YPLLs lost, worldwide14Percent of all DALYs lost, worldwide14Percent of all YPLLs lost, Europe14Percent of all DALYs lost, Europe14Percent of all YPLLs lost, US and Canada14Percent of all DALYs lost, US and Canada14Infectious and parasitic diseases, especially lower respiratory tract infections, diarrhea, AIDS, tuberculosis, and malaria37%26%9%6%5%3%Neuropsychiatric conditions, e.g. depression2%13%3%19%5%28%Injuries, especially motor vehicle accidents14%12%18%13%18%10%Cardiovascular diseases, principally heart attacks and stroke14%10%35%23%26%14%Premature birth and other perinatal deaths11%8%4%2%3%2%Cancer8%5%19%11%25%13% Main article: Preventive medicine Many diseases and disorders can be prevented through a variety of means. These include sanitation, proper nutrition, adequate exercise, vaccinations, and other self-care and public health measures. Main article: Therapy Medical therapies or treatments are efforts to cure or improve a disease or other health problem. In the medical field, therapy is synonymous with the word treatment. Among psychologists, the term may refer specifically to psychotherapy or "talk therapy". Common treatments include medications, surgery, medical devices, and self-care. Treatments may be provided by an organized health care system, or informally, by the patient or family members. A prevention or preventive therapy is a way to avoid an injury, sickness, or disease in the first place. A treatment or cure is applied after a medical problem has already started. A treatment attempts to improve or remove a problem, but treatments may not produce permanent cures, especially in chronic diseases. Cures are a subset of treatments that reverse diseases completely or end medical problems permanently. Many diseases that cannot be completely cured are still treatable. Pain management (also called pain medicine) is that branch of medicine employing an interdisciplinary approach to the relief of pain and improvement in the quality of life of those living with pain15 Treatment for medical emergencies must be provided promptly, often through an emergency department or, in less critical situations, through an urgent care facility. Main article: Epidemiology Epidemiology is the study of the factors that cause or encourage diseases. Some diseases are more common in certain geographic areas, among people with certain genetic or socioeconomic characteristics, or at different times of the year. Epidemiology is considered a cornerstone methodology of public health research, and is highly regarded in evidence-based medicine for identifying risk factors for disease. In the study of communicable and non-communicable diseases, the work of epidemiologists ranges from outbreak investigation to study design, data collection and analysis including the development of statistical models to test hypotheses and the documentation of results for submission to peer-reviewed journals. Epidemiologists also study the interaction of diseases in a population, a condition known as a syndemic. Epidemiologists rely on a number of other scientific disciplines such as biology (to better understand disease processes), biostatistics (the current raw information available), Geographic Information Science (to store data and map disease patterns) and social science disciplines (to better understand proximate and distal risk factors). In studying diseases, epidemiology faces the challenge of defining them. Especially for poorly understood diseases, different groups might use significantly different definitions. Without an agreed-upon definition, different researchers will find very different numbers of cases and characteristics of the disease.16 Obesity was a status symbol in Renaissance culture: "The Tuscan General Alessandro del Borro", attributed to Andrea Sacchi, It is now generally regarded as a disease. How a society responds to diseases is the subject of medical sociology. A condition may be considered to be a disease in some cultures or eras but not in others. For example, obesity can represent wealth and abundance, and is a status symbol in famine-prone areas and some places hard-hit by HIV/AIDS.18 Epilepsy is considered a sign of spiritual gifts among the Hmong people.19 Sickness confers the social legitimization of certain benefits, such as illness benefits, work avoidance, and being looked after by others. The person who is sick takes on a social role called the sick role. A person who responds to a dreaded disease, such as cancer, in a culturally acceptable fashion may be publicly and privately honored with higher social status.20 In return for these benefits, the sick person is obligated to seek treatment and work to become well once more. As a comparison, consider pregnancy, which is not usually interpreted as a disease or sickness, even if the mother and baby may both benefit from medical care. Most religions grant exceptions from religious duties to people who are sick. For example, one whose life would be endangered by fasting on Yom Kippur or during Ramadan is exempted from the requirement, or even forbidden from participating. People who are sick are also exempted from social duties. For example, ill health is the only socially acceptable reason for an American to refuse an invitation to the White House.21 The identification of a condition as a disease, rather than as simply a variation of human structure or function, can have significant social or economic implications. The controversial recognitions as diseases of repetitive stress injury (RSI) and post-traumatic stress disorder (also known as "Soldier's heart", "shell shock", and "combat fatigue") has had a number of positive and negative effects on the financial and other responsibilities of governments, corporations and institutions towards individuals, as well as on the individuals themselves. The social implication of viewing aging as a disease could be profound, though this classification is not yet widespread. Lepers were people who were historically shunned because they had an infectious disease, and the term "leper" still evokes social stigma. Fear of disease can still be a widespread social phenomenon, though not all diseases evoke extreme social stigma. Social standing and economic status affect health. Diseases of poverty are diseases that are associated with poverty and low social status; diseases of affluence are diseases that are associated with high social and economic status. Which diseases are associated with which states varies according to time, place, and technology. Some diseases, such as diabetes mellitus, may be associated with both poverty (poor food choices) and affluence (long lifespans and sedentary lifestyles), through different mechanisms. The term diseases of civilization describes diseases that are more common among older people. For example, cancer is far more common in societies in which most members live until they reach the age of 80 than in societies in which most members die before they reach the age of 50. An illness narrative is a way of organizing a medical experience into a coherent story that illustrates the sick individual's personal experience. People use metaphors to make sense of their experiences with disease. The metaphors move disease from an objective thing that exists to an affective experience. The most popular metaphors draw on military concepts: Disease is an enemy that must be feared, fought, battled, and routed. The patient or the healthcare provider is a warrior, rather than a passive victim or bystander. The agents of communicable diseases are invaders; non-communicable diseases constitute internal insurrection or civil war. Because the threat is urgent, perhaps a matter of life and death, unthinkably radical, even oppressive, measures are society's and the patient's moral duty as they courageously mobilize to struggle against destruction. The War on Cancer is an example of this metaphorical use of language.22 Another class of metaphors describes the experience of illness as a journey: The person travels to or from a place of disease, and changes himself, discovers new information, or increases his experience along the way. He may travel "on the road to recovery" or make changes to "get on the right track".22 Some are explicitly immigration-themed: the patient has been exiled from the home territory of health to the land of the ill, changing identity and relationships in the process.23 Some metaphors are disease-specific. Slavery is a common metaphor for addictions: The alcoholic is enslaved by drink, and the smoker is captive to nicotine. Some cancer patients treat the loss of their hair from chemotherapy as a metonymy or metaphor for all the losses caused by the disease.22 Some diseases are used as metaphors for social ills: "Cancer" is a common description for anything that is endemic and destructive in society, such as poverty, injustice, or racism. AIDS was seen as a divine judgment for moral decadence, and only by purging itself from the "pollution" of the "invader" could society become healthy again.22 Authors in the 19th century commonly used tuberculosis as a symbol and a metaphor for transcendence. Victims of the disease were portrayed in literature as having risen above daily life to become ephemeral objects of spiritual or artistic achievement. In the 20th century, after its cause was better understood, the same disease became the emblem of poverty, squalor, and other social problems.23
. DISEASE. From Wikipedia, the free encyclopedia. It has been suggested that Illness be merged into this article or section. (Discuss) Proposed since May Medical condition redirects here. For medical condition terminology, see Medical state. For other uses, see Disease (disambiguation). A disease is an abnormal condition affecting the body of an organism. It is often construed to be a medical condition associated with specific symptoms and signs.1 It may be caused by external factors, such as infectious disease, or it may be caused by internal dysfunctions, such as autoimmune diseases. In humans, disease is often used more broadly to refer to any condition that causes pain, dysfunction, distress, social problems, or death to the person afflicted, or similar problems for those in contact with the person. In this broader sense, it sometimes includes injuries, disabilities, disorders, syndromes, infections, isolated symptoms, deviant behaviors, and atypical variations of structure and function, while in other contexts and for other purposes these may be considered distinguishable categories. Diseases usually affect people not only physically, but also emotionally, as contracting and living with many diseases can alter one s perspective on life, and their personality. Death due to disease is called death by natural causes. There are four main types of disease: pathogenic disease, deficiency disease, hereditary disease, and physiological disease. Diseases can also be classified as communicable and non-communicable disease. In many cases, the terms disease, disorder, morbidity and illness are used interchangeably.2 In some situations, specific terms are considered preferable. The term disease broadly refers to any condition that impairs normal function. Commonly, this term is used to refer specifically to infectious diseases, which are clinically evident diseases that result from the presence of pathogenic microbial agents, including viruses, bacteria, fungi, protozoa, multicellular organisms, and aberrant proteins known as prions. An infection that does not and will not produce clinically evident impairment of normal functioning, such as the presence of the normal bacteria and yeasts in the gut, is not considered a disease; by contrast, an infection that is asymptomatic during its incubation period, but expected to produce symptoms later, is usually considered a disease. Non-infectious diseases are all other diseases, including most forms of cancer, heart disease, and genetic disease. Illness and sickness are generally used as synonyms for disease.3 However, this term is occasionally used to refer specifically to the patient s personal experience of their disease.45 In this model, it is possible for a person to be diseased without being ill (to have an objectively definable, but asymptomatic, medical condition), and to be ill without being diseased (such as when a person perceives a normal experience as a medical condition, or medicalizes a non-disease situation in his or her life). Illness is often not due to infection but a collection of evolved responses, sickness behavior, by the body which aids the clearing of infection. Such aspects of illness can include lethargy, depression, anorexia, sleepiness, hyperalgesia, and inability to concentrate.678. In medicine, a disorder is a functional abnormality or disturbance. Medical disorders can be categorized into mental disorders, physical disorders, genetic disorders, emotional and behavioral disorders, and functional disorders. The term disorder is often considered more value-neutral and less stigmatizing than the terms disease or illness, and therefore is preferred terminology in some circumstances. In mental health, the term mental disorder is used as a way of acknowledging the complex interaction of biological, social, and psychological factors in psychiatric conditions. However, the term disorder is also used in many other areas of medicine, primarily to identify physical disorders that are not caused by infectious organisms, such as metabolic disorders. A medical condition is a broad term that includes all diseases and disorders. While the term medical condition generally includes mental illnesses, in some contexts the term is used specifically to denote any illness, injury, or disease except for mental illnesses. The Diagnostic and Statistical Manual of Mental Disorders (DSM), the widely used psychiatric manual that defines all mental disorders, uses the term general medical condition to refer to all diseases, illnesses, and injuries except for mental disorders.9 This usage is also commonly seen in the psychiatric literature. Some health insurance policies also define a medical condition as any illness, injury, or disease except for psychiatric illnesses.10. As it is more value-neutral than terms like disease, the term medical condition is sometimes preferred by people with health issues that they do not consider to be deleterious. On the other hand, by emphasizing the medical nature of the condition, this term is sometimes rejected, such as by proponents of the autism rights movement. The term medical condition is used as a synonym for medical state, where it describes a patient s current state, as seen from a medical standpoint. This usage is seen in statements that describe a patient as being in critical condition , for example. Morbidity (from Latin morbidus, meaning sick, unhealthy ) is a diseased state, disability, or poor health due to any cause.11 The term may be used to refer to the existence of any form of disease, or to the degree that the health condition affects the patient. Among severely ill patients, the level of morbidity is often measured by ICU scoring systems. Comorbidity is the simultaneous presence of two or more medical conditions, such as schizophrenia and substance abuse. In epidemiology and actuarial science, the term morbidity rate can refer to either the incidence rate, or the prevalence of a disease or medical condition. This measure of sickness is contrasted with the mortality rate of a condition, which is the proportion of people dying during a given time interval. Syndrome (from Ancient Greek syn, meaning together , and dramein, meaning run ) is a set of symptoms occurring together. Predisease is a type of or medicalization in which currently healthy people with risk factors for disease, but no evidence of actual disease, are told that they are sick. Prediabetes and prehypertension are common examples. Labeling a healthy person with predisease can result in overtreatment, such as taking drugs that only help people with severe disease, or in useful preventive measures, such as motivating the person to get a healthful amount of physical exercise.12. Flareup redirects here. For the Transformers character, see Flareup (Transformers). In an infectious disease, the incubation period is the time between infection and the appearance of symptoms. The latency period is the time between infection and the ability of the disease to spread to another person, which may precede, follow, or be simultaneous with the appearance of symptoms. Some viruses also exhibit a dormant phase, called viral latency, in which the virus hides in the body in an inactive state. For example, varicella zoster virus causes chickenpox in the acute phase; after recovery from chickenpox, the virus may remain dormant in nerve cells for many years, and later cause herpes zoster (shingles). A cure is the end of a medical condition or a treatment that is very likely to end it, while remission refers to the disappearance, possibly temporarily, of symptoms. Complete remission is the best possible outcome for incurable diseases. A flare-up can refer to either the recurrence of symptoms or an onset of more severe symptoms. A refractory disease is a disease that resists treatment, especially an individual case that resists treatment more than is normal for the specific disease in question. Progressive disease is a disease whose typical natural course is the worsening of the disease until death, serious debility, or organ failure occurs. Slowly progressive diseases are also chronic diseases; many are also degenerative diseases. The opposite of progressive disease is stable disease or static disease: a medical condition that exists, but does not get better or worse. A localized disease is one that affects only one part of the body, such as athlete s foot or an eye infection. A disseminated disease has spread to other parts; with cancer, this is usually called metastatic disease. A systemic disease is a disease that affects the entire body, such as influenza or high blood pressure. Main article: Transmission (medicine) Only some diseases such as influenza are contagious and commonly believed to be infectious. The micro-organisms that cause these diseases are known as pathogens and include varieties of bacteria, viruses, protozoa and fungi. Infectious diseases can be transmitted, e.g. by hand-to-mouth contact with infectious material on surfaces, by bites of insects or other carriers of the disease, and from contaminated water or food (often via faecal contamination), etc. In addition, there are sexually transmitted diseases. In some cases, micro-organisms that are not readily spread from person to person play a role, while other diseases can be prevented or ameliorated with appropriate nutrition or other lifestyle changes. Some diseases, such as most (but not all) forms of cancer, heart disease and mental disorders, are non-infectious diseases. Many non-infectious diseases have a partly or completely genetic basis (see genetic disorder) and may thus be transmitted from one generation to another. Social determinants of health are the social conditions in which people live which determine their health. Illnesses are generally related to social, economic, political, and environmental circumstances. Social determinants of health have been recognized by several health organizations such as the Public Health Agency of Canada and the World Health Organization to greatly influence collective and personal well-being. The World Health Organization s Social Determinants Council also recognizes Social determinants of health in poverty. When the cause of a disease is poorly understood, societies tend to mythologize the disease or use it as a metaphor or symbol of whatever that culture considers to be evil. For example, until the bacterial cause of tuberculosis was discovered in 1882, experts variously ascribed the disease to heredity, a sedentary lifestyle, depressed mood, and overindulgence in sex, rich food, or alcohol—all the social ills of the time.13. Disease burden is the impact of a health problem in an area measured by financial cost, mortality, morbidity, or other indicators. There are several measures used to quantify the burden imposed by diseases on people. The years of potential life lost (YPLL) is a simple estimate of the number of years that a person s life was shortened due to a disease. For example, if a person dies at the age of 65 from a disease, and would probably have lived until age 80 without that disease, then that disease has caused a loss of 15 years of potential life. YPLL measurements do not account for how disabled a person is before dying, so the measurement treats a person who dies suddenly and a person who died at the same age after decades of illness as equivalent. In 2004, the World Health Organization calculated that 932 million years of potential life were lost to premature death.14. The quality-adjusted life year (QALY) and disability-adjusted life year (DALY) metrics are similar, but take into account whether the person was healthy after diagnosis. In addition to the number of years lost due to premature death, these measurements add part of the years lost to being sick. Unlike YPLL, these measurements show the burden imposed on people who are very sick, but who live a normal lifespan. A disease that has high morbidity, but low mortality, will have a high DALY and a low YPLL. In 2004, the World Health Organization calculated that 1.5 billion disability-adjusted life years were lost to disease and injury.14. Disease categoryPercent of all YPLLs lost, worldwide14Percent of all DALYs lost, worldwide14Percent of all YPLLs lost, Europe14Percent of all DALYs lost, Europe14Percent of all YPLLs lost, US and Canada14Percent of all DALYs lost, US and Canada14Infectious and parasitic diseases, especially lower respiratory tract infections, diarrhea, AIDS, tuberculosis, and malaria37%26%9%6%5%3%Neuropsychiatric conditions, e.g. depression2%13%3%19%5%28%Injuries, especially motor vehicle accidents14%12%18%13%18%10%Cardiovascular diseases, principally heart attacks and stroke14%10%35%23%26%14%Premature birth and other perinatal deaths11%8%4%2%3%2%Cancer8%5%19%11%25%13% Main article: Preventive medicine. Many diseases and disorders can be prevented through a variety of means. These include sanitation, proper nutrition, adequate exercise, vaccinations, and other self-care and public health measures. Main article: Therapy. Medical therapies or treatments are efforts to cure or improve a disease or other health problem. In the medical field, therapy is synonymous with the word treatment. Among psychologists, the term may refer specifically to psychotherapy or talk therapy . Common treatments include medications, surgery, medical devices, and self-care. Treatments may be provided by an organized health care system, or informally, by the patient or family members. A prevention or preventive therapy is a way to avoid an injury, sickness, or disease in the first place. A treatment or cure is applied after a medical problem has already started. A treatment attempts to improve or remove a problem, but treatments may not produce permanent cures, especially in chronic diseases. Cures are a subset of treatments that reverse diseases completely or end medical problems permanently. Many diseases that cannot be completely cured are still treatable. Pain management (also called pain medicine) is that branch of medicine employing an interdisciplinary approach to the relief of pain and improvement in the quality of life of those living with pain15. Treatment for medical emergencies must be provided promptly, often through an emergency department or, in less critical situations, through an urgent care facility. Main article: Epidemiology. Epidemiology is the study of the factors that cause or encourage diseases. Some diseases are more common in certain geographic areas, among people with certain genetic or socioeconomic characteristics, or at different times of the year. Epidemiology is considered a cornerstone methodology of public health research, and is highly regarded in evidence-based medicine for identifying risk factors for disease. In the study of communicable and non-communicable diseases, the work of epidemiologists ranges from outbreak investigation to study design, data collection and analysis including the development of statistical models to test hypotheses and the documentation of results for submission to peer-reviewed journals. Epidemiologists also study the interaction of diseases in a population, a condition known as a syndemic. Epidemiologists rely on a number of other scientific disciplines such as biology (to better understand disease processes), biostatistics (the current raw information available), Geographic Information Science (to store data and map disease patterns) and social science disciplines (to better understand proximate and distal risk factors). In studying diseases, epidemiology faces the challenge of defining them. Especially for poorly understood diseases, different groups might use significantly different definitions. Without an agreed-upon definition, different researchers will find very different numbers of cases and characteristics of the disease.16. Obesity was a status symbol in Renaissance culture: The Tuscan General Alessandro del Borro , attributed to Andrea Sacchi, It is now generally regarded as a disease. How a society responds to diseases is the subject of medical sociology. A condition may be considered to be a disease in some cultures or eras but not in others. For example, obesity can represent wealth and abundance, and is a status symbol in famine-prone areas and some places hard-hit by HIV/AIDS.18 Epilepsy is considered a sign of spiritual gifts among the Hmong people.19. Sickness confers the social legitimization of certain benefits, such as illness benefits, work avoidance, and being looked after by others. The person who is sick takes on a social role called the sick role. A person who responds to a dreaded disease, such as cancer, in a culturally acceptable fashion may be publicly and privately honored with higher social status.20 In return for these benefits, the sick person is obligated to seek treatment and work to become well once more. As a comparison, consider pregnancy, which is not usually interpreted as a disease or sickness, even if the mother and baby may both benefit from medical care. Most religions grant exceptions from religious duties to people who are sick. For example, one whose life would be endangered by fasting on Yom Kippur or during Ramadan is exempted from the requirement, or even forbidden from participating. People who are sick are also exempted from social duties. For example, ill health is the only socially acceptable reason for an American to refuse an invitation to the White House.21. The identification of a condition as a disease, rather than as simply a variation of human structure or function, can have significant social or economic implications. The controversial recognitions as diseases of repetitive stress injury (RSI) and post-traumatic stress disorder (also known as Soldier s heart , shell shock , and combat fatigue ) has had a number of positive and negative effects on the financial and other responsibilities of governments, corporations and institutions towards individuals, as well as on the individuals themselves. The social implication of viewing aging as a disease could be profound, though this classification is not yet widespread. Lepers were people who were historically shunned because they had an infectious disease, and the term leper still evokes social stigma. Fear of disease can still be a widespread social phenomenon, though not all diseases evoke extreme social stigma. Social standing and economic status affect health. Diseases of poverty are diseases that are associated with poverty and low social status; diseases of affluence are diseases that are associated with high social and economic status. Which diseases are associated with which states varies according to time, place, and technology. Some diseases, such as diabetes mellitus, may be associated with both poverty (poor food choices) and affluence (long lifespans and sedentary lifestyles), through different mechanisms. The term diseases of civilization describes diseases that are more common among older people. For example, cancer is far more common in societies in which most members live until they reach the age of 80 than in societies in which most members die before they reach the age of 50. An illness narrative is a way of organizing a medical experience into a coherent story that illustrates the sick individual s personal experience. People use metaphors to make sense of their experiences with disease. The metaphors move disease from an objective thing that exists to an affective experience. The most popular metaphors draw on military concepts: Disease is an enemy that must be feared, fought, battled, and routed. The patient or the healthcare provider is a warrior, rather than a passive victim or bystander. The agents of communicable diseases are invaders; non-communicable diseases constitute internal insurrection or civil war. Because the threat is urgent, perhaps a matter of life and death, unthinkably radical, even oppressive, measures are society s and the patient s moral duty as they courageously mobilize to struggle against destruction. The War on Cancer is an example of this metaphorical use of language.22. Another class of metaphors describes the experience of illness as a journey: The person travels to or from a place of disease, and changes himself, discovers new information, or increases his experience along the way. He may travel on the road to recovery or make changes to get on the right track .22 Some are explicitly immigration-themed: the patient has been exiled from the home territory of health to the land of the ill, changing identity and relationships in the process.23. Some metaphors are disease-specific. Slavery is a common metaphor for addictions: The alcoholic is enslaved by drink, and the smoker is captive to nicotine. Some cancer patients treat the loss of their hair from chemotherapy as a metonymy or metaphor for all the losses caused by the disease.22. Some diseases are used as metaphors for social ills: Cancer is a common description for anything that is endemic and destructive in society, such as poverty, injustice, or racism. AIDS was seen as a divine judgment for moral decadence, and only by purging itself from the pollution of the invader could society become healthy again.22 Authors in the 19th century commonly used tuberculosis as a symbol and a metaphor for transcendence. Victims of the disease were portrayed in literature as having risen above daily life to become ephemeral objects of spiritual or artistic achievement. In the 20th century, after its cause was better understood, the same disease became the emblem of poverty, squalor, and other social problems.23.")
31
Definice nemoci Objektivní a subjektivní aspekty nemoci
Rozdílné přístupy k jejich měření Nemoc lze pojímat z mnoha aspektů. Jako objektivně zjistitelnou poruchu zdraví, kterou lze diagnostikovat a klasifikovat, která má své příčiny i podmínky a typický průběh, jejž lze do určité míry ovlivnit. Pro většinu lidí je nemoc spojena s vnímanými nesnázemi, které se stávají podnětem pro vyhledání pomoci (Žáček, 1974)
")
32
Schéma přirozené historie nemoci
Zdroj: Žáček

36
Teoretická východiska měření zdraví a nemoci
Kvalita života, koncept positivního zdraví, koncept sociálního zdraví (Kebza 2005) Koncepty zdraví (WHO 1946, disease, illness, Drbal, Bowling, Illich, Křivohlavý) Duševní zdraví Nemoc (nemocnost) Objektivní přístupy (statistiky, zdravotnická dokumentace, údaje o spotřebě péče) Subjektivní přístupy (dotazníková šetření, Euroqol) Měření zdravotního stavu ve vztahu ke kvalitě života „Burden of disease“, Healthy life years (HLY) – zdravé roky života
 Koncepty zdraví (WHO 1946, disease, illness, Drbal, Bowling, Illich, Křivohlavý) Duševní zdraví. Nemoc (nemocnost) Objektivní přístupy (statistiky, zdravotnická dokumentace, údaje o spotřebě péče) Subjektivní přístupy (dotazníková šetření, Euroqol) Měření zdravotního stavu ve vztahu ke kvalitě života. „Burden of disease , Healthy life years (HLY) – zdravé roky života.")
37
Mezinárodní klasifikace nemocí*
I Některé infekční a parazitární nemoci II. Novotvary III. Nemoci krve, krvetvorných orgánu, poruchy imunity IV. Nemoci endokrinní, výživy, přeměny látek V. Poruchy duševní VI. Nemoci nervové soustavy VI. Nemoci oka VIII. Nemoci ucha IX. Nemoci oběhové soustavy X. Nemoci dýchací soustavy XI. Nemoci trávící soustavy XII. Nemoci kůže XIII. Nemoci svalové a kosterní soustavy XIV. Nemoci močové a pohlavní XV. Těhotenství, porod a šestinedělí XVI. Některé stavy vzniklé v perinatálním období XVII. Vrozené vady XVIII, Příznaky, znaky a abnormální nálezy jinde nezařazené XIX. Poranění, otravy XX. Vnější příčina nemocnosti a úmrtnosti XXI. Faktory ovlivňující zdravotní stav a kontakt se zdravotnickými službami Přesnou klasifikaci nemocí komplikuje fakt, že etiologicky různé nemoci mohou způsobovat stejné nebo téměř stejné potíže (či vůbec projevy), a naopak že tatáž nemoc (etiologická příčina) se může v konkrétních případech projevovat různými způsoby a působit různé potíže. Mezinárodní zdravotnická organizace (WHO) se snaží tento pohled zohlednit tím, že kromě Mezinárodní statistická klasifikace nemocí a souvisejících zdravotních problémů (MKN, anglicky ICD, The International Statistical Classification of Diseases and Related Health Problems) v roce 2001 vydala i novou klasifikaci ICF (obtížně přeložitelný název The International Classification of Functioning, Disability and Health v češtině bývá uváděn jako Mezinárodní klasifikace funkčních schopností, disability a zdraví, Mezinárodní klasifikace funkční zdatnosti atd.) Ta se však zaměřuje především na tělesné problémy spadající do oblasti fyzioterapie. Psychiatrie v analýze spíše stagnuje. Třetí, navazující klasifikace se týká léčebných a adaptačních intervencí (International Classification of Health Interventions, ICHI) Do aktualizací MKN se promítá rozvoj našich poznatků o příčinách, vzniku a průběhu nemocí.
, a naopak že tatáž nemoc (etiologická příčina) se může v konkrétních případech projevovat různými způsoby a působit různé potíže. Mezinárodní zdravotnická organizace (WHO) se snaží tento pohled zohlednit tím, že kromě Mezinárodní statistická klasifikace nemocí a souvisejících zdravotních problémů (MKN, anglicky ICD, The International Statistical Classification of Diseases and Related Health Problems) v roce 2001 vydala i novou klasifikaci ICF (obtížně přeložitelný název The International Classification of Functioning, Disability and Health v češtině bývá uváděn jako Mezinárodní klasifikace funkčních schopností, disability a zdraví, Mezinárodní klasifikace funkční zdatnosti atd.) Ta se však zaměřuje především na tělesné problémy spadající do oblasti fyzioterapie. Psychiatrie v analýze spíše stagnuje. Třetí, navazující klasifikace se týká léčebných a adaptačních intervencí (International Classification of Health Interventions, ICHI) Do aktualizací MKN se promítá rozvoj našich poznatků o příčinách, vzniku a průběhu nemocí.")
38
Vybrané demografické ukazatele
Celková úmrtnost a její vývoj Specifická úmrtnost vztažena ke skupinám nemocí (Mezinárodní klasifikace nemocí) Dětská úmrtnost S pomocí těchto ukazatelů jsou reflektovány rozdíly (health gap, mezera ve zdraví), které jsou dokladem nerovností ve zdraví Nutnost standardizace těchto demografických dat ve vztahu ke stanoveným mezinárodním standardům (jinak by nebylo možné mezinárodní srovnání) Předpokládaná délka dožití (life expectancy) Mnoho mezinárodních srovnání vývoje zdravotního stavu vychází z těchto demografických ukazatelů úUdaje o vývoji nemocnosti jsou totiž méně dostupné Až nově jsou zpracovávány Světovou zdravotnickou organizací údaje o celkové zátěži nemocemi (budrden of disease)
 Dětská úmrtnost. S pomocí těchto ukazatelů jsou reflektovány rozdíly (health gap, mezera ve zdraví), které jsou dokladem nerovností ve zdraví. Nutnost standardizace těchto demografických dat ve vztahu ke stanoveným mezinárodním standardům (jinak by nebylo možné mezinárodní srovnání) Předpokládaná délka dožití (life expectancy) Mnoho mezinárodních srovnání vývoje zdravotního stavu vychází z těchto demografických ukazatelů. úUdaje o vývoji nemocnosti jsou totiž méně dostupné. Až nově jsou zpracovávány Světovou zdravotnickou organizací údaje o celkové zátěži nemocemi (budrden of disease)")
39
Kde je problém? Je v ČR starších občanů moc nebo málo?
Z politického a veřejného diskurzu v ČR by mohlo vyplývat, že nám hrozí stárnutí společnosti. Z hlediska srovnání s ostatními státy je to jinak, lidé u nás umírají dříve. Zdroj: WHO Heatlh data

40
Frekvence výskytu nových onemocnění roste s věkem, po 50. roku věku
Analýza incidence a úmrtnosti na ZN (C00 – C97) ve věkových skupinách (ČR, 1999) Pramen: převzato z ÚZIS
 ve věkových skupinách (ČR, 1999) Pramen: převzato z ÚZIS.")
41
Epidemiologie Vědní obor, který studuje rozložení a determinanty stavů a událostí majících vztah ke zdraví v určených populačních skupinách a využívá výsledků tohoto studia ke zvládnutí zdravotních problémů. Tato definice zahrnuje všechny dosavadní epidemiologické metody a současně je dobrým základem pro rozvoj nových přístupů, a to jak v tradiční medicínské oblasti, tak v celé sociální realitě při využití poznatků i jiných oborů.

42
Epidemiologie Incidence - míra frekvence, s jakou dochází v určitém časovém intervalu (obvykle v roce) ke vzniku nových onemocnění. Rozeznává se jednak incidence absolutní, zachycující počet nových případů nemoci ve stanoveném intervalu, jednak incidenci relativní (standardizovaná), kdy se počet nových případů nemoci vztahuje k počtu osob v exponované populaci.
, kdy se počet nových případů nemoci vztahuje k počtu osob v exponované populaci.")
43
Epidemiologie Prevalence – Podává informaci o rozsahu (objemu) nemocí v populaci. Z časového hlediska je to průřezový ukazatel zachycující počet existujících nemocí k určitému datu.

44
Modifikace Harvardského modelu incidence a prevalence nemocí ve vztahu k úmrtnosti
Příklad aplikace tohoto modelu např. v oblasti nádorových nemocí (incidence, prevalence, úmrtnost) Determinanty zdraví POPULACE PREVALENCE zdravotnické služby ZEMŘELÍ Podpora zdraví INCIDENCE uzdravení úmrtnost specifická úmrtnost
 Determinanty zdraví. POPULACE. PREVALENCE. zdravotnické služby. ZEMŘELÍ. Podpora. zdraví. INCIDENCE. uzdravení. úmrtnost. specifická úmrtnost.")
45
Vývoj incidence, úmrtnosti a prevalence ZN slinivky břišní v ČR (muži, v letech 1970 – 1998)
Zdroj: ÚZIS, Praha 45

46
Vývoj incidence, úmrtnosti a prevalence ZN průdušnice, průdušky a plic v ČR (muži, v letech 1970 – 1998) Zdroj: ÚZIS, Praha 46

47
Koncept burden of disease
Koncept „Burden of Disease“ předkládá srovnávací index zatížení nemocí či úrazem, pojmenovaný DALYs ( disability-adjusted life years- disabilitou ve vztahu k věku) a důsledku předčasné smrti nebo roků života s disabilitou.
 a důsledku předčasné smrti nebo roků života s disabilitou.")
48
Burden of disease Burden of disease (koncept hodnocení zátěže populace nemocností). Složený ukazatel pro měření zdravotního stavu obyvatelstva, využívající ukazatelů nemocnosti, úmrtnosti a různých omezujících důsledků nemocí z hlediska společenské seberealizace či neschopnosti péče o sebe sama (nesoběstačnost, disaptibilita) k celkovému hodnocení zdravotního stavu populace. Tento složený ukazatel vyjadřuje disabilitu (sníženou míru uplatnění) jedinců v letech života (Disability Adjusted Life Years – DALY). Metodický přístup tohoto konceptu byl použit v několika studiích Světové zdravotnické organizace pro celkové mezinárodně srovnávací hodnocení zdravotního stavu (Murray a Lopez, 1994). Metoda byla postupně vypracována v posledních 18 letech a není zatím běžně používána na národní úrovni, i když jde nepochybně o velice hodnotný zdroj informací o celkové zatíženosti sledované populace komplexními důsledky nemoci. Jde o propočet, který zohledňuje roky ztraceného života v důsledku předčasného úmrtí v kombinaci s roky života, jejichž kvalita byla omezena v důsledku charakteru disaptibility. Metoda DALY je však zajímavá z hlediska cíle, který sleduje, tj. celkové hodnocení zdravotního stavu s využitím jediného složeného ukazatele. Její větší význam a možnost využití spočívají v současnosti zejména v kontextu mezinárodního srovnání.
. Složený ukazatel pro měření zdravotního stavu obyvatelstva, využívající ukazatelů nemocnosti, úmrtnosti a různých omezujících důsledků nemocí z hlediska společenské seberealizace či neschopnosti péče o sebe sama (nesoběstačnost, disaptibilita) k celkovému hodnocení zdravotního stavu populace. Tento složený ukazatel vyjadřuje disabilitu (sníženou míru uplatnění) jedinců v letech života (Disability Adjusted Life Years – DALY). Metodický přístup tohoto konceptu byl použit v několika studiích Světové zdravotnické organizace pro celkové mezinárodně srovnávací hodnocení zdravotního stavu (Murray a Lopez, 1994). Metoda byla postupně vypracována v posledních 18 letech a není zatím běžně používána na národní úrovni, i když jde nepochybně o velice hodnotný zdroj informací o celkové zatíženosti sledované populace komplexními důsledky nemoci. Jde o propočet, který zohledňuje roky ztraceného života v důsledku předčasného úmrtí v kombinaci s roky života, jejichž kvalita byla omezena v důsledku charakteru disaptibility. Metoda DALY je však zajímavá z hlediska cíle, který sleduje, tj. celkové hodnocení zdravotního stavu s využitím jediného složeného ukazatele. Její větší význam a možnost využití spočívají v současnosti zejména v kontextu mezinárodního srovnání.")
49
Burden of disease Koncept Burden of disease byl použit Světovou bankou a WHO při vypracování studie GBD 1990, jejímiž základními cíli bylo: oddělit epidemiologické hodnocení rozsahu zdravotních problémů od prosazování zájmů jednotlivých zdravotních plánů nebo intervencí; zahrnout do mezinárodní diskuse o zdravotní politice společný náhled na informace o nemocnosti a úmrtnosti; změřit zdravotní problémy v časových jednotkách (rocích) použitelných při ekonomických výpočtech; šlo o rozsáhlou studii, zaměřenou na posouzení zdraví světové populace, která poskytuje tyto informace: stupeň škod na zdraví vyplývajících z předčasné úmrtnosti a nemocnosti, příspěvek rozličných nemocí, úrazů a rizikových faktorů k celkové úrovni zdraví, krátkodobé a střednědobé projekce předčasných úmrtí a nemocnosti.
 použitelných při ekonomických výpočtech; šlo o rozsáhlou studii, zaměřenou na posouzení zdraví světové populace, která poskytuje tyto informace: stupeň škod na zdraví vyplývajících z předčasné úmrtnosti a nemocnosti, příspěvek rozličných nemocí, úrazů a rizikových faktorů k celkové úrovni zdraví, krátkodobé a střednědobé projekce předčasných úmrtí a nemocnosti.")
50
Roky života prožité ve zdraví (HLY), státy EU 15 + ČR, muži
Zdroj: Core health indicators from World health report, WHO, 2005.

51
Souhrnné ukazatele zdraví metodiky Burden of Disease
DALY (disability-adjusted life years lost) patří k ukazatelům měřících rozdíl mezi skutečným zdravím populace a určitým definovaným cílem (jde o počet roků života populace ztracených předčasnými úmrtími a nemocností). Je součtem složky popisující ztráty zdraví způsobené předčasnými úmrtími - years of life lost a složky popisující ztráty způsobené nemocností
 patří k ukazatelům měřících rozdíl mezi skutečným zdravím populace a určitým definovaným cílem (jde o počet roků života populace ztracených předčasnými úmrtími a nemocností). Je součtem složky popisující ztráty zdraví způsobené předčasnými úmrtími - years of life lost a složky popisující ztráty způsobené nemocností.")
54
Koncept „burden of disease“
Burden of Disease statistics (related to WHO's burden of disease activities) Statistical measures relating to the burden of disease. Includes: Healthy Life Expectancy (HALE); Life Expectancy; Discussion Papers. Also, this is where to find manuals, resources and software for carrying out national burden of disease studies.Burden of Disease Project The Global Burden of Disease project: results for 1990 and 2000 to 2002, methods and documentation. Manuals, resources and software for carrying out national burden of disease studies. Global Burden of Disease Estimates Incidence, prevalence, mortality, YLL, YLD and DALYs by sex, cause and region, estimates for 2002 as reported in the World Health Reports 2003 and Healthy Life Expectancy Healthy life expectancy (HALE) is based on life expectancy (LEX), but includes an adjustment for time spent in poor health. This indicator measures the equivalent number of years in full health that a newborn child can expect to live based on the current mortality rates and prevalence distribution of health states in the population. Discussion papers Global Programme on Evidence for Health Policy - Discussion Papers LIFE TABLES AND METHODS Life Tables for 191 Countries Beginning with the year 1999, WHO began making annual life tables for all Member States. These life tables have several uses and form the basis of all WHO's estimates about mortality patterns and levels world-wide. A key use of these life tables is in the construction of healthy life expectancy (HALE) which is the basic indicator of population health levels used by WHO and published each year in the World Health Report. Modified Logit Life Table System The Modified Logit model life table system is a 2-parameter system based on the Brass logit model and using a global standard.
 Statistical measures relating to the burden of disease. Includes: Healthy Life Expectancy (HALE); Life Expectancy; Discussion Papers. Also, this is where to find manuals, resources and software for carrying out national burden of disease studies.Burden of Disease Project The Global Burden of Disease project: results for 1990 and 2000 to 2002, methods and documentation. Manuals, resources and software for carrying out national burden of disease studies. Global Burden of Disease Estimates Incidence, prevalence, mortality, YLL, YLD and DALYs by sex, cause and region, estimates for 2002 as reported in the World Health Reports 2003 and Healthy Life Expectancy Healthy life expectancy (HALE) is based on life expectancy (LEX), but includes an adjustment for time spent in poor health. This indicator measures the equivalent number of years in full health that a newborn child can expect to live based on the current mortality rates and prevalence distribution of health states in the population. Discussion papers Global Programme on Evidence for Health Policy - Discussion Papers. LIFE TABLES AND METHODS. Life Tables for 191 Countries Beginning with the year 1999, WHO began making annual life tables for all Member States. These life tables have several uses and form the basis of all WHO s estimates about mortality patterns and levels world-wide. A key use of these life tables is in the construction of healthy life expectancy (HALE) which is the basic indicator of population health levels used by WHO and published each year in the World Health Report. Modified Logit Life Table System The Modified Logit model life table system is a 2-parameter system based on the Brass logit model and using a global standard.")
55
QALY Quality Adjusted life year

56
Grafické znázornění QALY

57
Dva typy měření zdravotního stavu
Měření zdravotního stavu obyvatelstva jsou standardně realizována na základě dvou přístupů: využití rutinních statistických údajů a (2) měření nemocnosti pomocí výběrových šetření (výzkum) Výhodou rutinních statistických dat je, že tato data jsou dostupná v delších časových řadách.
 měření nemocnosti pomocí výběrových šetření (výzkum) Výhodou rutinních statistických dat je, že tato data jsou dostupná v delších časových řadách.")
58
Přístupy k měření zdravotního stavu a jeho determinant - souhrn
Statistická šetření Demografické údaje Střední délka života, úmrtnost celková, specifická, standardizace Zdravotní a sociální statistiky Národní onkologický registr Infekční onemocnění Invalidita, pracovní neschopnost Nezaměstnanost, příjmy, vzdělání Výzkum Epidemiologické studie (incidence, prevalence) Euroqol, SF36 Kvalita života Sociologická dotazníková šetření (sociální a ekon. determinanty:vzdělání,příjem; rizika:tabák, strava) Údaje zdravotních pojišťoven, údaje o spotřebě služeb Zdravotnická dokumentace
 Euroqol, SF36. Kvalita života. Sociologická dotazníková šetření (sociální a ekon. determinanty:vzdělání,příjem; rizika:tabák, strava) Údaje zdravotních pojišťoven, údaje o spotřebě služeb. Zdravotnická dokumentace.")
59
Typy ukazatelů pro měření zdraví a diskuse možností jejich využití pro tvorbu a realizaci zdravotní politiky Zdraví Kvalita života, dimenze zdraví Determinanty zdraví Poznání a kontrola determinant v konkrétních podmínkách daného státu, kontinentů, globálně Demografické procesy Dlouhodobé a střednědobé predikce vývoje a hodnocení důsledků pro zdravotní péči, rozhodování při tvorbě zdravotní politiky Nemocnost (epidemiologie) Možnosti využití pro plánování, organizaci a financování zdravotnických služeb, hodnocení potřeb Burden of disease (DALY) Možnosti mezinárodního srovnání, nezávislé na užším epidemiologickém přístupu, do kterého se mohou také snadněji promítat profesní přístupy. Kompozitní ukazatel však „zakrývá“ konkrétní problémy. QALY Používáno pro hodnocení dosahovaných výsledků, ekonomické studie
 Možnosti využití pro plánování, organizaci a financování zdravotnických služeb, hodnocení potřeb. Burden of disease (DALY) Možnosti mezinárodního srovnání, nezávislé na užším epidemiologickém přístupu, do kterého se mohou také snadněji promítat profesní přístupy. Kompozitní ukazatel však „zakrývá konkrétní problémy. QALY. Používáno pro hodnocení dosahovaných výsledků, ekonomické studie.")
60
Zdroje dat WHO Health data (volný přístup!!, ideální pro mezinárodní srovnání) Databáze Health for All (online, offline) ÚZIS, ČSÚ (ukázky) OECD Health Data (ukázka?)
 ÚZIS, ČSÚ. (ukázky) OECD Health Data. (ukázka )")
61
Demografie Možná literatura pro zájemce o studium demografie:
Pavlík, Z. Rychtaříková, J., Šubrtová, A.: Základy demografie. Academia, Praha 1986, 732 s., Roubíček, V.: Úvod do demografie. Codex Bohemia, Praha 1997, 349 s. Demografie (nejen) pro demografy. Sociologické nakladatelství a Sociologický ústav AV ČR, Praha 1993 Rabušic, L.: Česká společnost stárne. MU Brno, 1995 Časopis Demografie
 pro demografy. Sociologické nakladatelství a Sociologický ústav AV ČR, Praha Rabušic, L.: Česká společnost stárne. MU Brno, Časopis Demografie.")
62
Zdroj dat ČR – Národní onkologický registr Drogy – Evropa USA
Drogy – Evropa USA

63
Sociologie medicíny Pojem sociologie medicíny
V současnosti odpovídají předmětnému zaměření této subdisciplíny lépe pojmy: Sociologie zdraví a péče o zdraví Sociologie zdraví a nemoci Studium medicíny představuje pouze jednu část

64
Aktuální předmětné zaměření
1. social epidemiology 2. studies of development and organizational dynamics 3. The reaction of societies to illness, including meaning of normative expectations 4. The social policies, social movements, politics and economic conditions

65
Poznámky k historickému vývoji
50. léta Sociální determinanty zdraví, nerovnosti ve zdraví T.Parsons (1951), role nemocného, sociální role, význam pro fungování společnosti, nemocný je sankcionován (jistá podobnost s českou současností) Studium nemocí a lékařské péče v sociálním kontextu, struktura a funkce sociálních rolí Freidson (1970) Profession of Medicine Dominantní postavení lékařů
, role nemocného, sociální role, význam pro fungování společnosti, nemocný je sankcionován (jistá podobnost s českou současností) Studium nemocí a lékařské péče v sociálním kontextu, struktura a funkce sociálních rolí. Freidson (1970) Profession of Medicine. Dominantní postavení lékařů.")
66
Poznámky k historickému vývoji
60. léta Goffmanův koncept stigmatu

67
Poznámky k historickému vývoji
70. léta Rozvoj výzkumu v USA, zdroje financování (NIMH, NCHSR) Časopisy: Health Services Research, Medical Care Výzkum spotřeby zdravotnických služeb Chování ve vztahu ke zdraví Andersonův model (poměrně komplexní model) David Mechanic (stress a duševní zdraví) Journal of Health and Social Behavior
 Časopisy: Health Services Research, Medical Care. Výzkum spotřeby zdravotnických služeb. Chování ve vztahu ke zdraví. Andersonův model (poměrně komplexní model) David Mechanic (stress a duševní zdraví) Journal of Health and Social Behavior.")
68
Poptávka a nabídka zdravotní péče - Anderson
Faktory ovlivňující poptávku Zdravotní stav Hodnocení potřeb Nemocnost Detrminanty zdraví a nemoci vzdělání, příjem, životní styl, genetické vlohy, prostředí POTŘEBY Zdravotní péče Kvalita života Subjektivní pacientovy pocity POPTÁVKA Zdravotní péče Nabídkou vyvolaná poptávka Faktory ovlivňující nabídku Faktory ovlivňující nabídku SPOTŘEBA Zdravotní péče Medicínské technologie Rozhodnutí lékařů Management Možnosti substituce Alokace zdrojů Nákup služeb Metody úhrady Smluvní vztahy Zdravotní politika NABÍDKA Zdravotní péče

69
Poznámky k historickému vývoji
80. léta V USA změny ve financování, pokles vlivu lékařů, vznik Medicare, Medicaid a růst podnikatelského vlivu Omezení prostředků a sociologicky zaměřený výzkum Transformace NCHSR na Agency for Health Care Policy and Research Výzkumnými prioritami se stalo tlumení růstu nákladů, medicínská efektivita, medicína založená na důkazech (evidence-based medicine) Finance přesměrovány na ekonomiku, klinický výzkum a epidemiologii Sociologicky zaměřený výzkum byl fragmentován
 Finance přesměrovány na ekonomiku, klinický výzkum a epidemiologii. Sociologicky zaměřený výzkum byl fragmentován.")
70
Poznámky k historickému vývoji
90. léta Critical Medical Sociology Koncept medikalizace (Conrad, 1992) Pokračující výzkumy v oblasti stigmatu Wagnerův model řízení péče o chronicky nemocné Nerovnosti ve zdraví Mezinárodní srovnávací výzkumy Health policy research Neformální péče
 Pokračující výzkumy v oblasti stigmatu. Wagnerův model řízení péče o chronicky nemocné. Nerovnosti ve zdraví. Mezinárodní srovnávací výzkumy. Health policy research. Neformální péče.")
71
OECD 2001 (Ottawa) a další navazující práce 2000-2011
Hodnocení výsledků – performance measurement NEJDE JENOM O TECHNOLOGY ASSESSMENT WHO 2000, 2010 Health Systems: Improving Performance OECD 2001 (Ottawa) a další navazující práce Measuring Up Smith 2009 Performance Measurement for Health System Improvement. Cambridge University Press Kutzin 2010 Implementing Health Financing Reform. Lessons from countris in transition. WHO, European Observatory on Health Systems and Policies Reisman 2007 Health Care and Public Policy. Edward Elgar ukázka
 a další navazující práce Measuring Up. Smith Performance Measurement for Health System Improvement. Cambridge University Press. Kutzin Implementing Health Financing Reform. Lessons from countris in transition. WHO, European Observatory on Health Systems and Policies. Reisman Health Care and Public Policy. Edward Elgar. ukázka.")
72
Jako příklad lze uvést strukturaci předmětu hodnocení výsledků u Smith 2009
Principy performance measurement Dimensions of performance Population health Patient-reported outcome measures Measuring clinical quality Measuring financialprotectin Health system responsiveness Measuring equity and access Health systém productivity and efficiency

73
Případová studie Ukázka analýzy vývoje zdravotního stavu obyvatel Jihočeského kraje. Institut zdravotní politiky a ekonomiky 2002, Sborník č. 2/2002 Medical Sociology. M.K.Zimmerman Encyclopedia of Sociology. Eds. E.F. Borgatta, J.V.Rhonda Montgomery. Vol. 3, 2nd edit., New York, Macmillan Reference USA, 2001, p

74
Health 2020 Nová strategie péče o zdraví, zdravotní politiky v Evropském regionu WHO New Site Health 2020

78
Key components of Health 2020?
Values Health 2020 is based on the values enshrined in the WHO Constitution: the highest attainable standard of health as a human right. It acknowledges the interconnectedness of local, national, regional and global health actors, actions and challenges, and recommends a unity of approach and the adoption of a common outcome-focused Region-wide policy framework. It provides a clear mapping of the options and tradeoffs in taking action to improve health and reduce inequities.

79
key components of Health 2020
Health development Health is a resource that enables every person to realize his or her potential and to contribute to the overall development of society. The new policy framework does not imply that health is everything or the only aspect of life to be valued – societies and individuals have many goals. Yet health is crucial as a means to achieve other goals in life. Poor health wastes potential, causes despair and drains resources across all sectors of society.

80
key components of Health 2020
Problem-solving The policy framework presents ways in which policy-makers can more effectively and efficiently address today’s social, demographic, epidemiological and financial challenges, by resetting priorities, catalyzing action in other sectors, and adopting new approaches to organizing the health sector with other stakeholders. Engagement Many partners need to come together to achieve better and more equitable health and well-being, and health is the responsibility of the whole of society and the whole of government. The policy framework is designed to help overcome some of the principal barriers that have so far held back those with an interest in health. It provides a vision, a strategic path, a set of priorities and a range of suggestions to show what works in engaging stakeholders, based on research and experience in many countries.

81
key components of Health 2020
Equity focus The policy framework suggests new ways to identify important health gaps and focus individual and collective efforts on ways to reduce them. It shows how progress has been most successful in countries that provide affordable care and social safety nets through strong public services and sustainable public finances.

82
key components of Health 2020
Evidence base Health 2020 builds on the experiences gained from previous health for all policies and is supported by a wealth of evidence gathered in both traditional and emerging health policy areas. Strategic thinking The policy framework recognizes that governments can achieve real improvements in health if they work across government to fulfil two linked strategic objectives.

83
Health 2020 objectives The two strategic objectives are:
improving health for all and reducing health inequalities improving leadership and participatory governance for health.

85
Analýza zdravotního stavu obyvatelstva JČ kraje a jeho vývoje v členění podle okresů v porovnání s ČR a EU Cíle projektu: Orientační analýza zdravotních problémů obyvatelstva JČ kraje na úrovni okresů v porovnání s ČR a EU Stručný přehled výchozích teoretických poznatků z oblasti podpory zdraví a dosavadních zkušeností s jejich využitím při tvorbě a realizaci zdravotní politiky Diskuse prioritních zdravotních problémů ve vztahu ke společenským skupinám, geografickému rozdělení, k existujícím preventivním programům a potřebám dalších analýz a výzkumu. Institut zdravotní politiky a ekonomiky, 2000

86
Analýza demografického vývoje
Věková struktura obyvatelstva (okresy) Vývoj celkové úmrtnosti (EU, ČR) Celková úmrtnost (okresy) Střední délka života (okresy) Specifická úmrtnost (nádory, srdeční a cévní nemoci) – okresy, ČR Přehled okresů se zvýšenou úmrtností na nádory než průměr ČR
 Vývoj celkové úmrtnosti (EU, ČR) Celková úmrtnost (okresy) Střední délka života (okresy) Specifická úmrtnost (nádory, srdeční a cévní nemoci) – okresy, ČR. Přehled okresů se zvýšenou úmrtností na nádory než průměr ČR.")
87
Analýza demografického vývoje: věková struktura obyvatelstva v letech 1991 a (v %), celkem (podle stavu k ) 0 - 14 65+ 1991 2000 EU 15 18,3 x 17,0 43,0 24,0 13,5 x 16,0 ČR 20,6 16,2 44,5 43,5 22,2 26,4 12,7 13,9 Jihočeský kraj 21,1 16,6 45,2 43,8 21,4 25,9 12,0 13,6 České Budějovice 21,0 16,5 45,3 44,0 26,2 13,3 Český Krumlov 23,4 18,1 47,5 45,9 20,0 25,4 9,1 10,6 Jindřichův Hradec 21,7 44,9 43,6 20,7 25,5 Písek 20,2 42,4 22,3 26,3 15,3 Prachatice 22,5 17,4 46,3 45,1 20,3 25,3 10,9 12,2 Strakonice 20,1 16,1 48,0 43,2 22,1 19,3 14,4 Tábor 20,5 44,2 43,3 22,0 25,7 14,9 Poznámka: X – 1990, zdroj ČSÚ

88
Analýza vývoje celkové úmrtnosti v ČR a EU
Střední Evropa EU Skandinávské země Zdroj: WHO; Health data, (standardizováno na obyvatel)
")
89
Analýza rozdílů celkové standardizované úmrtnosti mezi okresy JČ kraje
Zdroj: ČSÚ, Praha

90
Analýza rozdílů celkové standardizované úmrtnosti mezi okresy JČ kraje a ČR (muži)
Český Krumlov Prachatice České Budějovice Tábor Zdroj: ČSÚ, Praha

91
Analýza rozdílů celkové standardizované úmrtnosti mezi okresy JČ kraje a ČR (ženy)
Český Krumlov Strakonice České Budějovice Písek Tábor Zdroj: ČSÚ, Praha

92
Střední délka života - muži
České Budějovice Tábor Prahatice Český Krumlov Zdroj: ČSÚ, Praha

93
Střední délka života - ženy
České Budějovice Tábor Strakonice Český Krumlov Zdroj: ČSÚ, Praha

94
Analýza rozdílů úmrtnosti na ZN tlustého střeva mezi okresy JČ kraje (muži, průměr 1991 - 1998)
Zdroj: ÚZIS, Praha (standardizováno na obyvatel a věkově na evropský standard)
")
95
Vývoj úmrtnosti na nemoci oběhové soustavy - analýza rozdílů mezi okresy JČ kraje
Zdroj: ČSÚ, Praha. Nemoci oběhové soustavy (I00 – I99)
")
96
Vývoj podílů úmrtnosti podle příčin smrti mezi lety 1990 a 2000 (muži a ženy v procentech)
")
97
Analýza nemocnosti Klasifikace zdravotních problémů
Hypertenzní nemoc, ICHS (prevalence v CŘ) Incidence a prevalence nádorových onemocnění Vybrané ZN s vyšší incidencí v jednotlivých okresech Prevalence nádorových onemocnění Analýza vývoje vztahů incidence, úmrtnosti a prevalence nádorových onemocnění
 Incidence a prevalence nádorových onemocnění. Vybrané ZN s vyšší incidencí v jednotlivých okresech. Prevalence nádorových onemocnění. Analýza vývoje vztahů incidence, úmrtnosti a prevalence nádorových onemocnění.")
98
Klasifikace zdravotních problémů v JČ kraji se zaměřením na možnosti prevence
Přehled skupin: Kardiovaskulární onemocnění Novotvary Cerebrovaskulární onemocnění Respirační nemoci Endokrinní a metabolické poruchy Duševní poruchy Orální zdraví Nemoci kosterní a svalové soustavy Neurologické poruchy Nemoci zažívacího traktu Sexuálně přenosné nemoci AIDS Úrazy Vrozené vady

99
Vývoj prevalence hypertenzní choroby v ČR
(prevalence na 1000 osob, srovnání výsledků různých šetření v letech 1982 – 1999) Studie celkem 0 - 14 75 + 1969 – 70 ÚSLOZ Balogh 74 M 65,2 0,5 23,0 Ž 99,4 7,8 C 83,1 15,0 1986 ÚZIS 70,0 106,9 88 – 89 ÚSLOZ (Urban 92) 140,1 1,3 12,9 35,6 80,7 261,2 331,6 351,5 359,9 176,7 5,8 12,7 10,3 70,1 269,1 458,3 509,8 484,1 159,9 HIS CR 93 (ÚZIS 95) 86,0 - 7 15 55 131 193 203 200 116,0 13 61 113 204 316 333 HIS CR 96 ÚZIS 129,0 3 17 75 236 280 419 142,0 14 68 144 228 421 369 HIS CR 99 ÚZIS 2001 118,0 8,0 11,0 21,0 149,0 293,0 303,0 276,0 152,0 10,0 60,0 156,0 278,0 454 351,0 Hodonín 2001 154,8 225,4
 Studie. celkem – 70 ÚSLOZ Balogh 74. M. 65,2. 0,5. 23,0. Ž. 99,4. 7,8. C. 83,1. 15, ÚZIS. 70,0. 106,9. 88 – 89 ÚSLOZ (Urban 92) 140,1. 1,3. 12,9. 35,6. 80,7. 261,2. 331,6. 351,5. 359,9. 176,7. 5,8. 12,7. 10,3. 70,1. 269,1. 458,3. 509,8. 484,1. 159,9. HIS CR 93 (ÚZIS 95) 86, , HIS CR 96 ÚZIS. 129, , HIS CR 99 ÚZIS ,0. 8,0. 11,0. 21,0. 149,0. 293,0. 303,0. 276,0. 152,0. 10,0. 60,0. 156,0. 278, ,0. Hodonín ,8. 225,4.")
100
Vývoj prevalence hypertenzní choroby (na 1000 osob v ČR v letech 1970 – 2001)
")
101
Prevalence hypertenzní nemoci ve věkových skupinách (okres Hodonín, 2001)
Zdroj: VZP Hodonín. Prevalence - absolutní počty

102
Mezinárodní srovnání vývoje celkové incidence novotvarů (standardizováno na 100 000 obyvatel)
Zdroj: WHO; Health data, (standardizováno na obyvatel)
")
103
Vývoj incidence ZN na 100 000 mužů (rozdíly mezi okresy JČ kraje a ČR)
Zdroj ÚZIS, Praha

104
Incidence ZN a novotvary in situ na 100 000 mužů (průměr let 1995-1999)
Zdroj ÚZIS; Praha 2001

105
Vývoj incidence ZN na 100 000 žen (rozdíly mezi okresy JČ kraje a ČR)
Zdroj ÚZIS, Praha

106
Incidence ZN a novotvary in situ na 100 000 žen (průměr let 1995-1999)
Zdroj ÚZIS; Praha 2001

107
Analýza incidence a úmrtnosti na ZN (C00 – C97) ve věkových skupinách (ČR, 1999)
Pramen: převzato z ÚZIS

108
Analýza podílu incidence ZN v ČR (1998 ženy v procentech)
Zdroj ÚZIS, Praha

109
Vývoj incidence, prevalence a úmrtnosti ZN tlustého střeva v okrese Tábor a v ČR - evropský standard - muži Zdroj ÚZIS, Praha

110
Analýza rozdílů incidence ZN průdušnice - trachey, průdušky - bronchu a plic mezi okresy JČ kraje (ženy, průměr ) Zdroj ÚZIS, Praha

111
Analýza rozdílů incidence a úmrtnosti ZN slinivky břišní mezi okresy JČ kraje (muži v letech ) Zdroj ÚZIS, Praha

112
Analýza rozdílů incidence a úmrtnosti ZN tlustého střeva mezi okresy JČ kraje (muži v letech ) Zdroj ÚZIS, Praha

113
Analýza rozdílů incidence a úmrtnosti ZN trachey, průdušky - bronchu a plíce mezi okresy JČ kraje (ženy v letech ) Zdroj ÚZIS, Praha

114
Analýza rozdílů incidence a úmrtnosti ZN těla děložního mezi okresy JČ kraje (ženy v letech ) Zdroj ÚZIS, Praha

115
Korelační analýza incidence ZN (C00 - C97) a SDŽ ve vybraných státech (za rok 1997)
Zdroj ČSÚ, ÚZIS, Praha

116
Vývoj prevalence vybraných ZN v ČR (v letech 1991 až 1998 na 100 tis
Vývoj prevalence vybraných ZN v ČR (v letech 1991 až 1998 na 100 tis. mužů) Zdroj: ÚZIS, Praha
 Zdroj: ÚZIS, Praha.")
117
Prevalence vybraných ZN v ČR (ve věkových skupinách mužů, 1998)
Zdroj: ÚZIS, Praha

118
Vývoj incidence, úmrtnosti a prevalence ZN slinivky břišní v ČR (muži, v letech 1970 – 1998)
Zdroj: ÚZIS, Praha

119
Vývoj incidence, úmrtnosti a prevalence ZN průdušnice, průdušky a plic v ČR (muži, v letech 1970 – 1998) Zdroj: ÚZIS, Praha

120
Vývoj incidence, úmrtnosti a prevalence ZN průdušnice, průdušky a plic v ČR (ženy, v letech 1970 – 1998) Zdroj: ÚZIS, Praha

121
Vývoj incidence, úmrtnosti a prevalence ZN melanomu kůže v ČR (ženy, v letech 1970 – 1998)
Zdroj: ÚZIS, Praha

122
Demografická projekce kraje Vysočina
Jako vstupní parametry projekce byla použita data Českého statistického úřadu, konkrétně: krajské specifické míry plodnosti žen kraje Vysočina v roce 2000 (úhrnná plodnost dosáhla v tomto roce hodnoty 1,17) řády vymírání z úmrtnostních tabulek pro kraj Vysočina za období (střední délka života při narození činila 72,7 roku u mužů a 78,7 roku u žen) struktura obyvatelstva Vysočiny podle pohlaví, jednotek věku a podle okresů, bilancovaná k na stav 518 315 obyvatel. Byly uvažovány dvě varianty dalšího vývoje plodnosti: nižší - plodnost takřka neporoste, v roce 2020 uvažována úhrnná plodnost na úrovni 1,20; vyšší - plodnost mírně poroste, v roce 2020 uvažovaná úroveň plodnosti 1,45.
 řády vymírání z úmrtnostních tabulek pro kraj Vysočina za období (střední délka života při narození činila 72,7 roku u mužů a 78,7 roku u žen) struktura obyvatelstva Vysočiny podle pohlaví, jednotek věku a podle okresů, bilancovaná k na stav obyvatel. Byly uvažovány dvě varianty dalšího vývoje plodnosti: nižší - plodnost takřka neporoste, v roce 2020 uvažována úhrnná plodnost na úrovni 1,20; vyšší - plodnost mírně poroste, v roce 2020 uvažovaná úroveň plodnosti 1,45.")
123
Roční přírůstky (úbytky) obyvatelstva v kraji Vysočina v základních produktivních skupinách (výchozí stav k projekce do roku 2020 pro obě varianty plodnosti) Zdroj: Projekce obyvatelstva kraje Vysočina do roku Praha: Katedra demografie VŠE, 2003.

124
Kumulovaný přírůstek počtu obyvatel v kraji Vysočina v základních produktivních skupinách (výchozí stav k projekce do roku 2020 pro obě varianty plodnosti) Zdroj: Projekce obyvatelstva kraje Vysočina do roku Praha: Katedra demografie VŠE, 2003.

126
Závěry 1. Vývoj zdravotního stavu a jeho determinant je jedním z klíčových východisek tvorby a realizace zdravotní politiky jak na národní tak regionální a lokální úrovni Pro hodnocení vývoje zdravotního stavu máme k dispozici celou řadu teoretických poznatků, metod měření zdraví a souvisejících dat (epidemiologie, statistiky, demografie, burden of disease) NEVYUŽITÉ MOŽNOSTI: V ČR se údaje o vývoji zdravotního stavu pro tvorbu a realizaci zdravotní politiky využívají poměrně málo, pro výzkum a analýzy nemocnosti nejsou využita data zdravotních pojišťoven a rovněž není v potřebném rozsahu využita metoda výběrových šetření
 NEVYUŽITÉ MOŽNOSTI: V ČR se údaje o vývoji zdravotního stavu pro tvorbu a realizaci zdravotní politiky využívají poměrně málo, pro výzkum a analýzy nemocnosti nejsou využita data zdravotních pojišťoven a rovněž není v potřebném rozsahu využita metoda výběrových šetření.")
127
Závěry 2. V procesech nastolení agendy zdravotní politiky ještě pořád převládají témata z oblasti financování, vlastnictví, organizace, obchodu, apod. Větší dostupnost údajů je v oblasti úmrtnosti, méně pak v oblasti nemocnosti – tento trend platí obecně na mezinárodní úrovni. Determinanty zdraví nejsou kontrolovatelné jenom na individuální úrovni medicíny, větší význam má naopak populační přístup, je zapotřebí důkazy podložená kombinace obou přístupů.

128
Model vztahů vybraných aspektů přípravy zdravotního plánu kraje

129
Informace pro studenty
Seminární práce ze zdravotní politiky Informace jsou uvedeny na Na stejné adrese jsou také ukázky prací studentů

130
Doplňují informace k seminární práci studentů
Návrh možnosti pracovat také v týmu Možná témata: Analýza procesu „Agenda setting“ české zdravotní politiky ve vybraném časovém úseku, případně srovnání se Slovenskou republikou Sociologie medicíny – souhrn jejího vývoje, přehled témat, která řeší Je však zapotřebí, aby byl jasně vymezen autorský podíl jednotlivých členů týmu (pro potřeby hodnocení)
")
Podobné prezentace

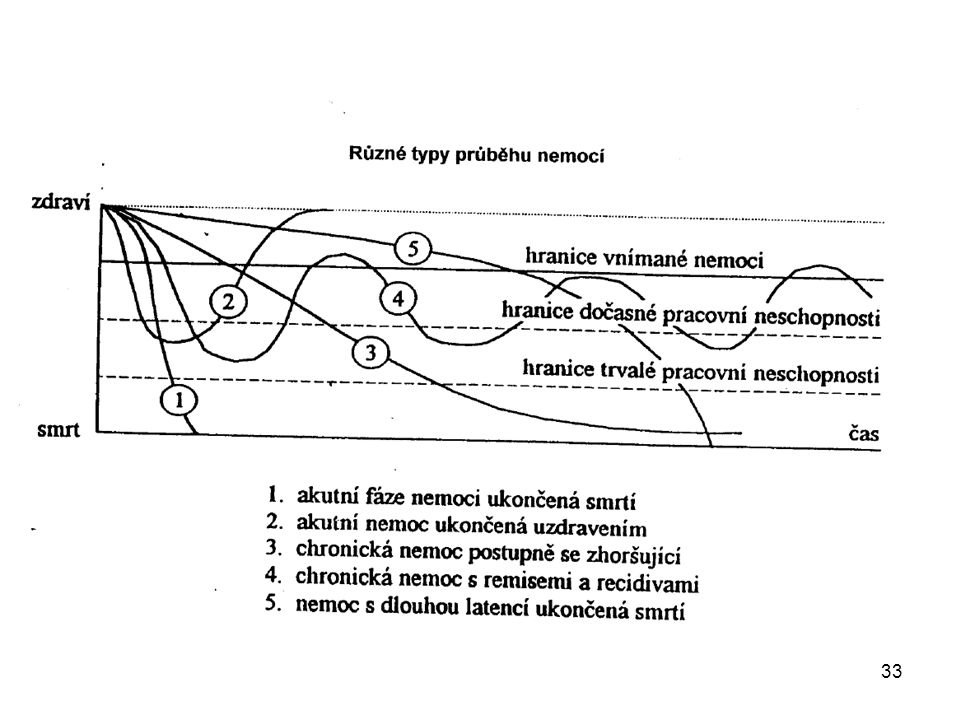
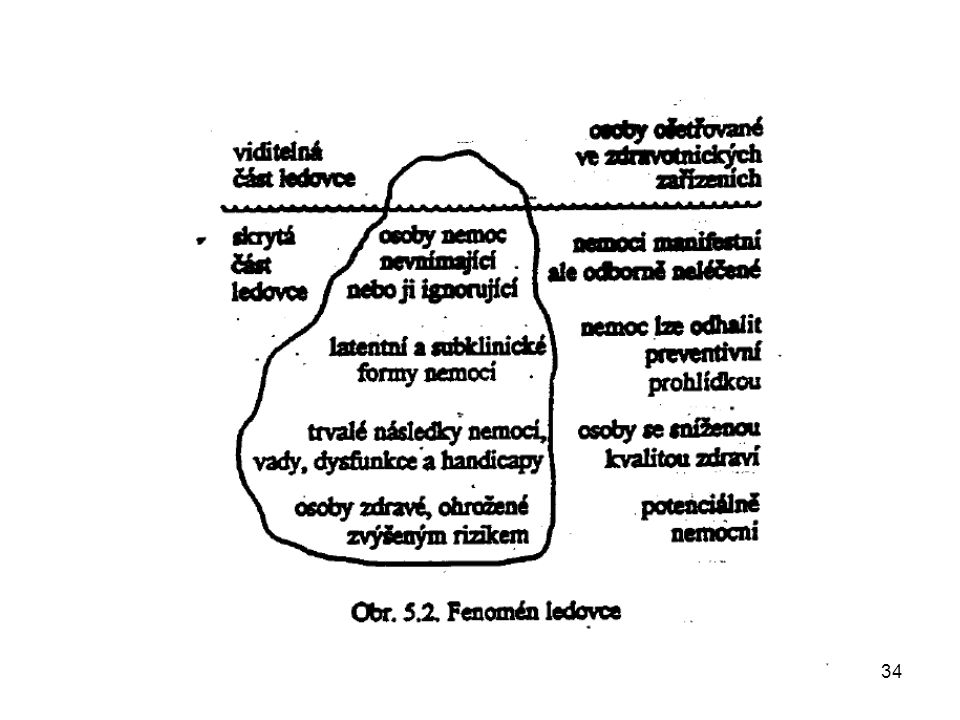
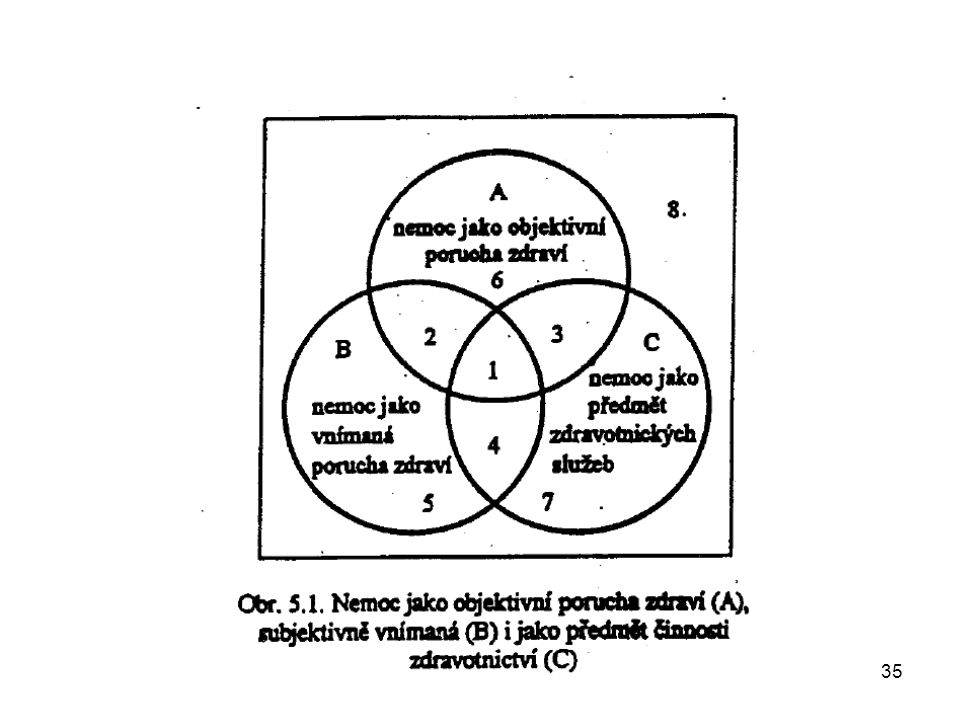
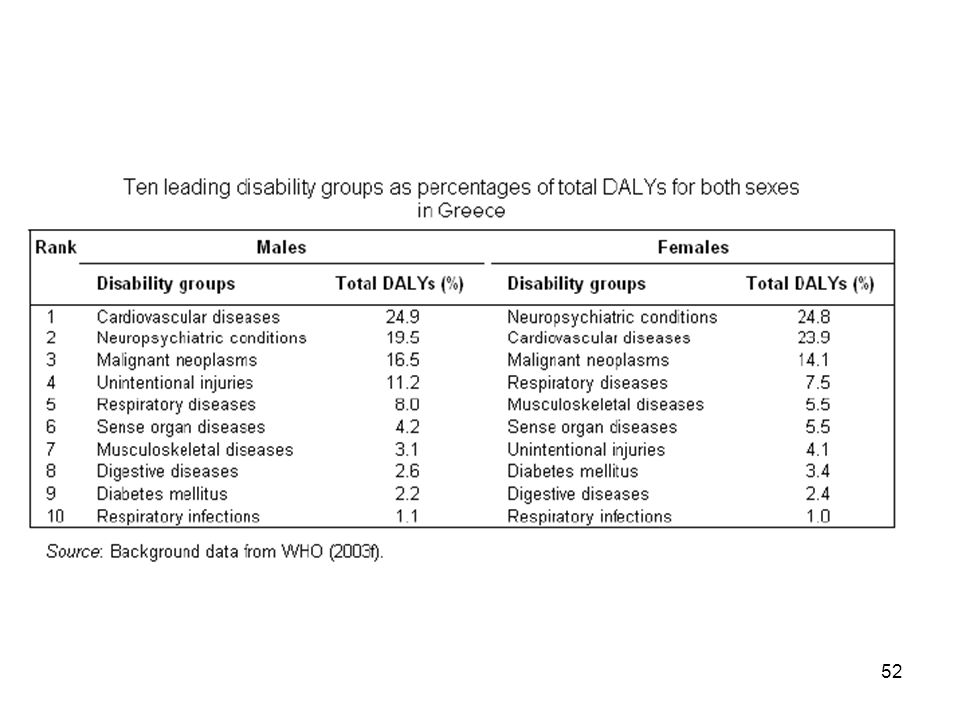


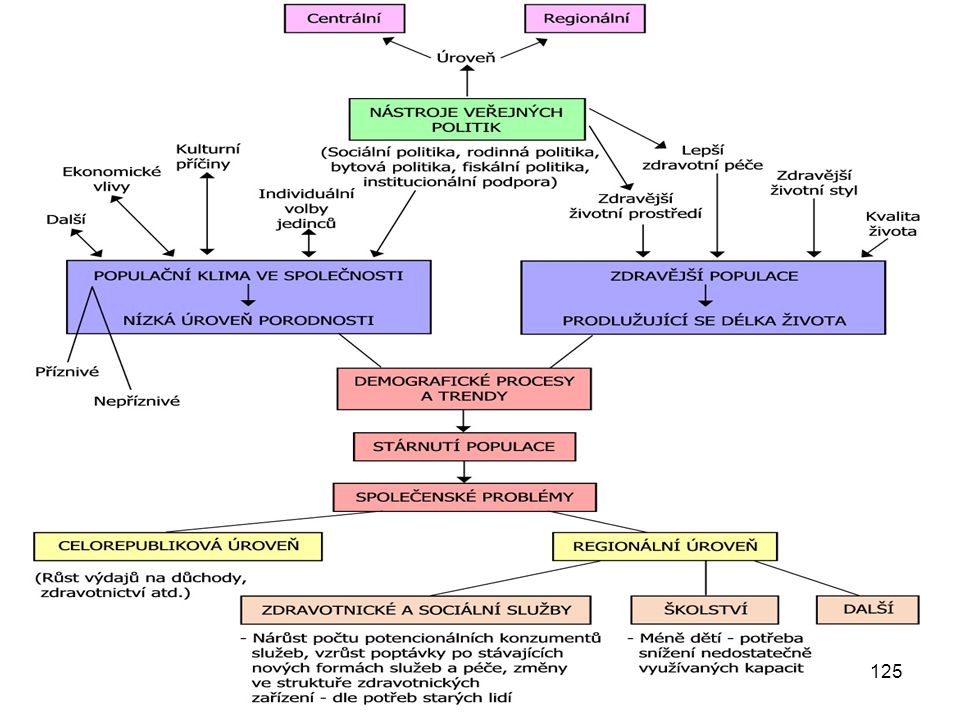
![Vyhodnocení dotazníku – Barcamp Brno 2013 Magdaléna Katolická magdalena [at] marketingovevyzkumy.cz](/7/1904186/big_thumb.jpg "Vyhodnocení dotazníku – Barcamp Brno 2013 Magdaléna Katolická magdalena [at] marketingovevyzkumy.cz>")













>")




